


Nearly every conversation about HPV centers on the cervix — but roughly 7% of American adults carry an oral HPV infection right now, and most of them have no idea. If you have just learned that you or a partner has oral HPV, or if you noticed a persistent throat symptom that sent you searching, the first thing to understand is this: the vast majority of oral HPV infections clear on their own within one to two years, without treatment and without causing any lasting harm. This article explains what oral HPV actually is, how it behaves, and what you can do to support your immune system through the process.
Key Takeaways
- Oral HPV infects the mouth, throat, tonsils, and base of the tongue — and most infections produce zero symptoms.
- Approximately 7% of U.S. adults have oral HPV at any given time; about 1% carry a high-risk strain.
- Most oral HPV infections resolve naturally within one to two years through normal immune function.
- High-risk strains like HPV-16 are linked to oropharyngeal cancer only after many years of persistent, uncleared infection — a positive result is not a cancer diagnosis.
- There is no routine approved screening test for oral HPV; immune support, lifestyle changes, and regular clinical follow-up are the primary tools available.
In This Article
- What is oral HPV?
- How common is oral HPV?
- How oral HPV spreads
- Symptoms — and why most people have none
- High-risk strains and cancer risk
- Who is more likely to have persistent oral HPV?
- How oral HPV is diagnosed
- How to support natural clearance
- Does the HPV vaccine help?
- When to see a doctor
- Frequently asked questions
What Is Oral HPV?
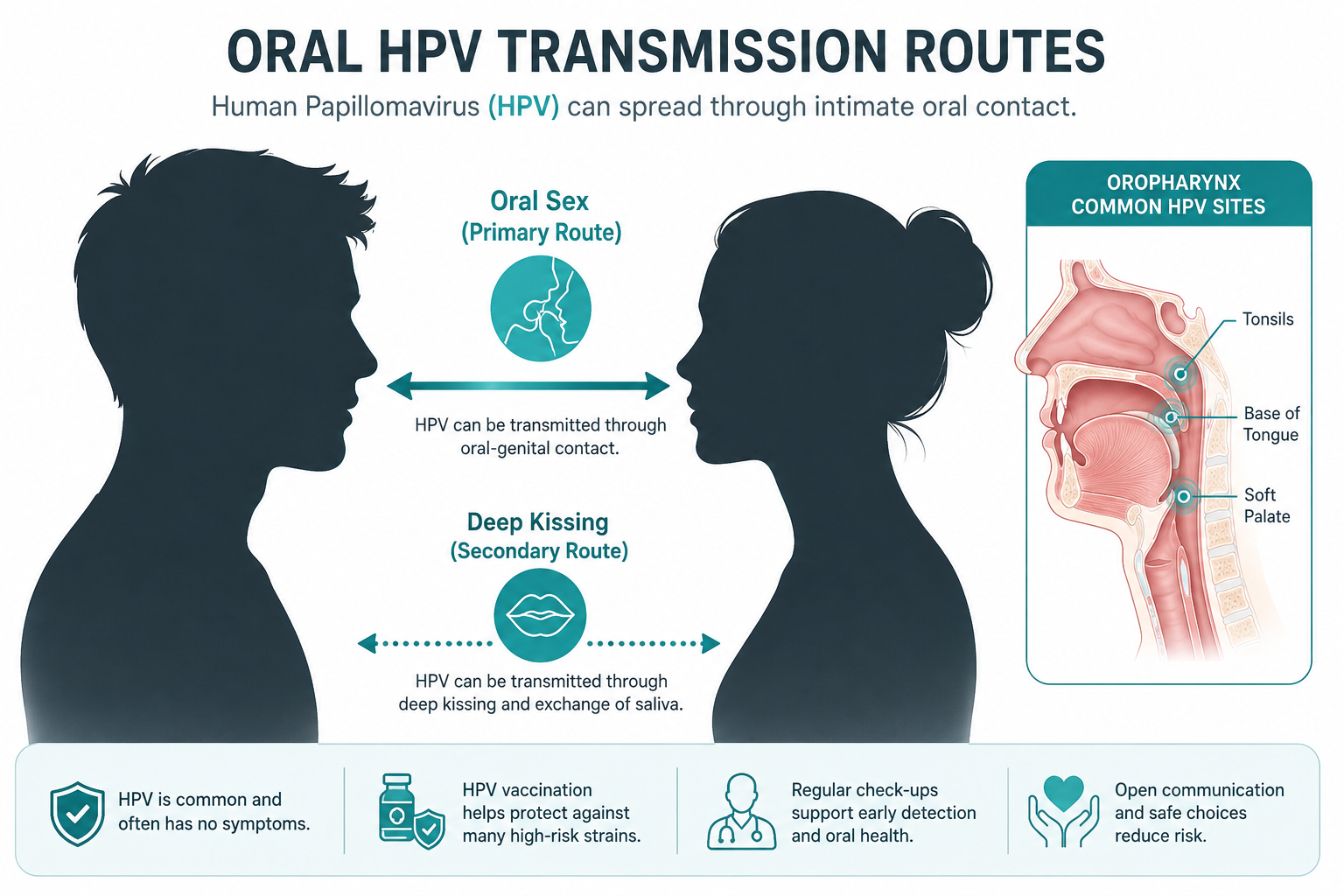
Oral HPV is an infection caused by the human papillomavirus that takes hold in the tissues of the mouth, throat, tonsils, or base of the tongue. It is the same pathogen responsible for genital HPV — the difference is location, not the virus itself.
More than 200 distinct HPV types have been identified. The majority are classified as low-risk, meaning they do not cause cancer. A smaller subset — roughly a dozen types — are considered high-risk because of their association with certain cancers when the infection persists over a long period. When HPV infects oral tissues, it typically enters through microscopic breaks in the mucosal lining, where it can establish a low-level infection that the immune system either clears or, in some cases, fails to fully eliminate.
The biology is straightforward: HPV is a DNA virus that infects epithelial cells. In the oral cavity, these are the cells lining the mouth and throat. The virus does not enter the bloodstream in a meaningful way. It lives locally, in the tissue, which is why immune function at the mucosal level matters so much for clearance.
How Common Is Oral HPV?
The prevalence figures are higher than most people expect. According to data from the Centers for Disease Control and Prevention, approximately 7% of U.S. adults between the ages of 14 and 69 carry an oral HPV infection at any given time. Of those, roughly 1% carry a high-risk oral strain.
Prevalence is not evenly distributed. Men have significantly higher rates of oral HPV than women — a pattern that holds across age groups and is thought to reflect differences in immune response and mucosal biology. Prevalence also increases with age, peaking in men between their 50s and 60s, which is one reason oropharyngeal cancer rates have shifted toward older males over the past two decades.
The most striking aspect of these numbers is that the overwhelming majority of infected individuals have no symptoms and no clinical diagnosis. They carry the virus, their immune system eventually clears it, and they never know it happened. For men specifically, this silent pattern is particularly relevant — the topic is explored in depth in HPV in men: no symptoms, no test, still at risk.
How Oral HPV Spreads
The primary transmission route for oral HPV is oral sex. This is the most well-documented pathway, supported by consistent epidemiological data. The risk increases with the number of oral sex partners, which aligns with what is known about HPV transmission generally.
Deep kissing has been proposed as a secondary route, and some studies suggest a modest association — but the evidence is less robust than for oral-genital contact. It is biologically plausible given that HPV can be present in saliva, but the transmission efficiency through kissing alone appears to be considerably lower.
Sharing items such as lip products, cigarettes, or utensils is theoretically possible but has not been well-documented in the literature. Casual contact — handshakes, shared surfaces, airborne exposure — does not transmit HPV. The virus requires direct mucosal or skin-to-skin contact to establish infection.
Being honest about what is and is not established matters here. Oral HPV is not a sign of unusual behavior. It is a common viral infection spread through a common sexual practice, and stigma around it is largely unwarranted.
Symptoms — and Why Most People Have None
The central clinical reality of oral HPV is that it is almost entirely asymptomatic. Most people who carry an oral HPV infection experience nothing — no pain, no visible changes, no throat discomfort. The infection exists below the threshold of awareness, and the immune system resolves it quietly.
When symptoms do appear, they are non-specific and overlap with many other, more common conditions. They can include:
- A persistent sore throat that does not resolve with standard treatment
- Hoarseness or a change in voice quality lasting more than two weeks
- A lump or swelling in the neck
- Difficulty swallowing
- White or red patches inside the mouth
- A mouth sore that does not heal within two to three weeks
- Unexplained ear pain
None of these symptoms should be interpreted as confirmation of oral HPV. Each of them has a long list of potential causes, most of which are benign. Self-diagnosis is not appropriate. Any symptom that persists beyond two weeks deserves clinical evaluation — not because it is likely to be serious, but because the only way to know is to have a clinician assess it.
High-Risk Strains and Cancer Risk
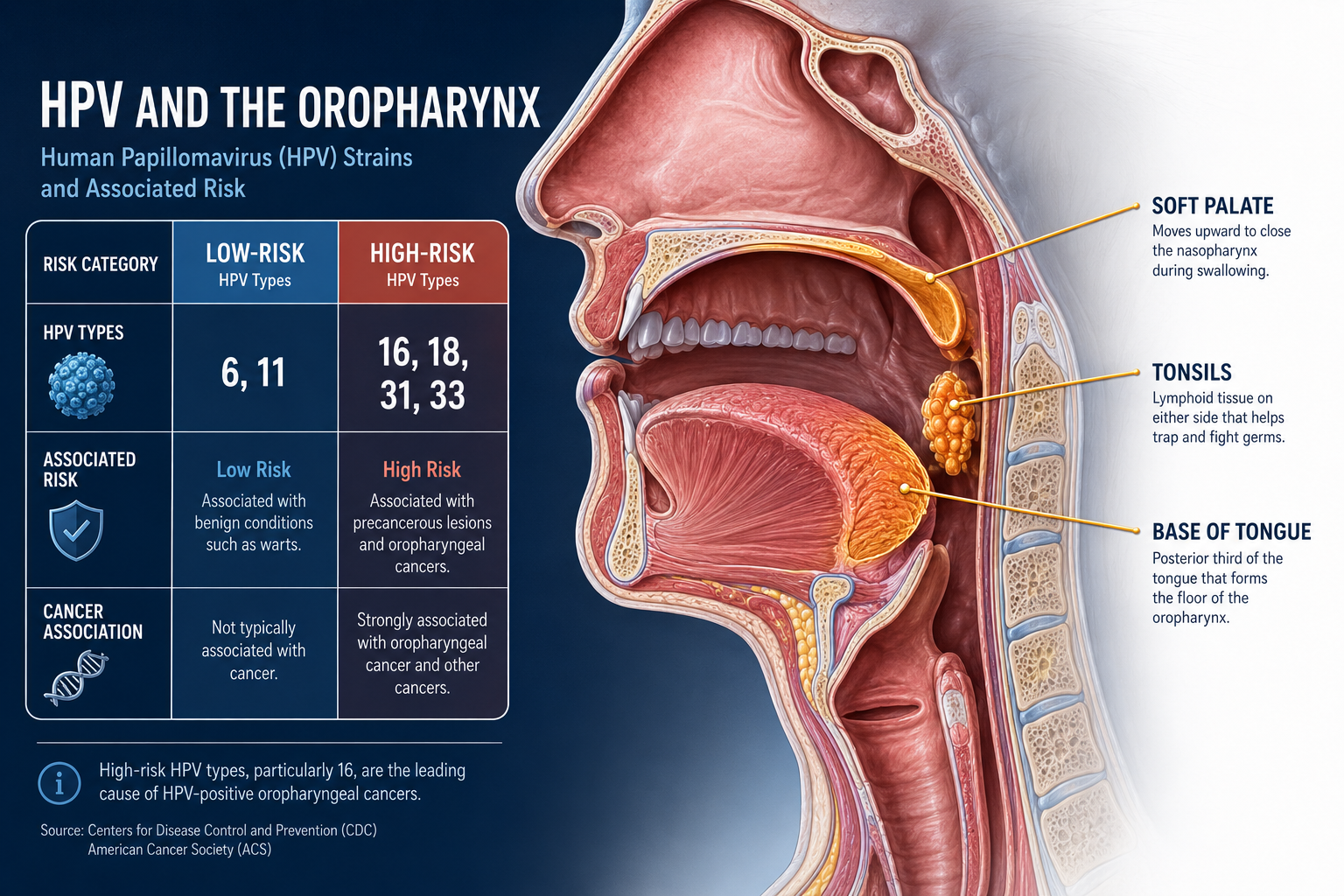
HPV-16 is the strain most strongly associated with oropharyngeal cancer — cancers involving the tonsils, the base of the tongue, and the back of the throat. According to the National Cancer Institute, HPV is now the leading cause of oropharyngeal cancers in the United States, surpassing tobacco in many demographic groups.
This requires careful framing. A positive oral HPV result — even for a high-risk strain — is not a cancer diagnosis. Cancer develops only when a high-risk infection persists for many years without clearance, and even then, additional cellular changes must occur. The vast majority of people who acquire HPV-16 orally will clear it without ever developing cancer. The risk is real, but it is a long-term, conditional risk — not an immediate one.
| HPV Strain Type | Examples | Primary Risk |
|---|---|---|
| Low-risk | 6, 11 | Oral warts; no cancer association |
| High-risk | 16, 18, 31, 33 | Oropharyngeal cancer if infection persists over many years |
For a detailed breakdown of why HPV-16 and HPV-18 carry higher oncogenic potential than other strains, see why HPV-16 and HPV-18 are the most dangerous HPV strains. That article covers the molecular mechanisms in full — the focus here is the oral context specifically.

Who Is More Likely to Have Persistent Oral HPV?
Most oral HPV infections clear. The ones that do not tend to occur in people whose immune systems are less able to mount an effective response. Several factors are consistently associated with higher persistence risk.
| Risk Factor | Mechanism / Impact on Clearance |
|---|---|
| Smoking | Damages mucosal immunity; strongly associated with HPV persistence |
| Heavy alcohol use | Impairs immune cell function; increases mucosal vulnerability |
| Immunosuppression (HIV, medications) | Reduces T-cell and NK-cell activity needed to clear HPV |
| Vitamin D deficiency | Associated with reduced innate and adaptive immune function |
| Chronic stress | Elevates cortisol, which suppresses immune surveillance |
| Poor sleep quality | Reduces cytokine production and immune cell regeneration |
| Multiple concurrent HPV strains | May overwhelm immune prioritization |
| Male sex | Men have higher oral HPV persistence rates than women across all age groups |
The interaction between these factors is cumulative. A smoker who is also sleep-deprived and vitamin D-deficient faces a meaningfully higher persistence risk than someone with only one of those factors present.
For a thorough examination of the biological and lifestyle reasons some people fail to clear HPV while others do not, why some people clear HPV faster than others covers the full picture.
How Oral HPV Is Diagnosed
There is no routine, approved screening test for oral HPV in the general population. This is a critical point that often surprises people. Unlike cervical HPV, which has well-established screening protocols through Pap smears and co-testing, oral HPV has no equivalent standard-of-care screening tool.
Diagnosis, when it occurs, happens through one of three pathways:
- Throat swab PCR testing — ordered by a clinician when symptoms warrant investigation. This can detect HPV DNA in oral samples but is not a standard screening tool.
- Visual examination — by a dentist, oral surgeon, or ENT specialist who identifies abnormal tissue changes during a routine or symptom-driven exam.
- Biopsy — performed when abnormal tissue is found and a definitive diagnosis is needed.
The practical implication is significant: most people with oral HPV are never formally diagnosed because they clear the virus without developing symptoms or tissue changes. The absence of a positive test does not mean the absence of infection — and the absence of symptoms does not mean the infection is not present.
How to Support Natural Clearance
No antiviral drug eliminates HPV. The immune system is the only mechanism through which the virus clears — which means that anything supporting immune function is directly relevant to clearance.
Lifestyle factors with the strongest evidence:
- Smoking cessation carries the most robust evidence for improving HPV clearance rates. Smoking is both a direct immunosuppressant and a mucosal irritant. Stopping is the single highest-impact action a person can take.
- Alcohol reduction matters because heavy drinking impairs the T-cell and natural killer cell activity that the immune system relies on to identify and eliminate HPV-infected cells.
- Vitamin D optimization is supported by NIH data on vitamin D and immune function, which shows its role in both innate and adaptive immune responses. Deficiency is common and correctable.
- Consistent sleep — seven to nine hours per night — allows the immune system to complete the cytokine signaling and cellular repair processes that daytime function disrupts.
- Stress management reduces chronic cortisol elevation, which is known to suppress immune surveillance.
On AHCC and HPV clearance:
AHCC (Active Hexose Correlated Compound) is the only supplement with a published, placebo-controlled human clinical trial specifically examining HPV clearance. The research was conducted by Dr. Judith Smith at the University of Texas Health Science Center at Houston. The study used 3 grams per day, taken on an empty stomach, over a minimum of six months. Results were promising, though the research is preliminary and AHCC is not FDA-approved as an HPV treatment.
NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility. At the research-validated dose of 3 grams per day, that equates to approximately four to five capsules daily, taken fasted. For a full review of the clinical evidence behind AHCC and HPV, does AHCC really help clear HPV covers the published research in detail. For dosing specifics, AHCC dosage for HPV provides the clinical protocol breakdown.
For a broader look at natural immune support strategies, how to clear HPV naturally covers the full range of evidence-based approaches.

Does the HPV Vaccine Help?
The HPV vaccine — Gardasil 9 — protects against nine HPV strains, including HPV-16 and HPV-18, which are responsible for the majority of HPV-associated oropharyngeal cancers. Vaccination prevents new infections from these strains. It does not clear an existing infection.
This distinction matters. If oral HPV is already present, the vaccine will not eliminate it. However, vaccination still offers meaningful protection against strains not yet acquired. Given that most sexually active adults have been exposed to some HPV types but not all, vaccination after partial exposure remains beneficial.
Current CDC recommendations support routine vaccination through age 26. For adults aged 27 to 45, the decision is made on a shared basis with a healthcare provider, weighing individual risk factors and likelihood of benefit.
When to See a Doctor
Most people with oral HPV will never need to see a specialist specifically for it — because most will clear the infection without ever knowing it was there. But certain symptoms should not be left unexamined.
See a clinician promptly if any of the following persist for more than two weeks:
- A sore throat that does not respond to standard treatment
- Hoarseness or a persistent change in voice quality
- A lump or swelling in the neck
- Difficulty swallowing
- A mouth sore that does not heal
- Unexplained ear pain on one side
- White or red patches inside the mouth or on the tongue
These symptoms are not automatically indicative of HPV or cancer. Most of the time, they have benign explanations. But two weeks is the clinical threshold at which further evaluation becomes appropriate, and no symptom in this list should be dismissed or monitored indefinitely without a professional assessment.
Frequently Asked Questions
Can you get oral HPV from kissing?
Deep kissing has been associated with oral HPV transmission in some studies, but the evidence is less consistent than for oral-genital contact. HPV can be present in saliva and oral mucosal cells, making transmission theoretically possible through sustained kissing. However, the efficiency of this route appears to be considerably lower than through oral sex. Casual kissing — a brief greeting kiss — has not been shown to be a meaningful transmission route.
Does oral HPV always cause cancer?
No. The overwhelming majority of oral HPV infections — including those caused by high-risk strains like HPV-16 — clear on their own without causing cancer or any other lasting harm. Cancer associated with oral HPV requires persistent infection over many years, combined with additional cellular changes. A positive oral HPV result is not a cancer diagnosis, and it should not be treated as one. The National Cancer Institute provides clear guidance on this distinction.
How do you know if you have oral HPV?
Most people do not know, because oral HPV typically causes no symptoms and there is no routine approved screening test for it. Diagnosis generally occurs only when symptoms prompt clinical investigation, or when a dentist or ENT identifies abnormal tissue during an examination. If you have concerns about oral HPV, speak with a healthcare provider about whether any evaluation is appropriate for your situation.
Can men get oral HPV?
Yes — and men actually have higher rates of oral HPV than women. According to CDC data, men are more likely to acquire oral HPV, more likely to carry high-risk strains, and less likely to clear the infection as efficiently as women. This is one reason why oropharyngeal cancers associated with HPV are more common in men. The full picture of how HPV presents differently in men is covered in HPV in men: no symptoms, no test, still at risk.
Does oral HPV go away on its own?
Yes, in most cases. Studies suggest that the majority of oral HPV infections clear within one to two years through normal immune function. The immune system recognizes HPV-infected cells and eliminates them over time — a process that happens silently in most people. Factors that can slow or prevent clearance include smoking, heavy alcohol use, immunosuppression, vitamin D deficiency, poor sleep, and chronic stress. Supporting immune function through these modifiable factors gives the body the best opportunity to clear the infection efficiently.
Conclusion: What to Do Next
Oral HPV is common, largely silent, and — for most people — self-resolving. The fear that often accompanies a diagnosis or a concerning symptom is understandable, but it is rarely proportionate to the actual clinical risk. The immune system is well-equipped to handle this virus. The goal is to make sure it has every advantage.
Concrete next steps:
- See your healthcare provider if you have persistent throat symptoms, a neck lump, or any of the warning signs listed above. Do not self-diagnose — get a clinical evaluation.
- Stop smoking if you smoke. This is the single most impactful action you can take for oral HPV clearance and for your overall mucosal immune health.
- Optimize the basics — sleep, vitamin D levels, alcohol intake, and stress management. These are not peripheral concerns; they directly affect how well your immune system functions.
- Ask about vaccination if you are under 45 and have not completed the HPV vaccine series. Even partial prior exposure does not eliminate the benefit of vaccination against strains not yet encountered.
- Consider evidence-based immune support — AHCC is the only supplement with a published human clinical trial for HPV clearance. If you are exploring supplementation, discuss it with your provider and review the available research before starting.
Related Reading
- Why HPV-16 and HPV-18 are the most dangerous HPV strains — A detailed look at the molecular reasons high-risk strains carry greater oncogenic potential.
- Does AHCC really help clear HPV? What the research actually says — A thorough review of the published clinical evidence for AHCC and HPV clearance.
- Why some people clear HPV faster than others — The biological and lifestyle factors that determine how quickly the immune system resolves an HPV infection.
- How to clear HPV naturally: 10 proven strategies — A comprehensive guide to evidence-based lifestyle and supplement strategies for supporting HPV clearance.
References
- Centers for Disease Control and Prevention. (2023). Human Papillomavirus (HPV). https://www.cdc.gov/hpv
- National Cancer Institute. (2023). HPV and Cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
- National Cancer Institute. (2022). Human Papillomavirus (HPV) and Cancer: Fact Sheet. https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-fact-sheet
- National Institutes of Health, Office of Dietary Supplements. (2023). Vitamin D: Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- Smith, J. A., et al. (2014). AHCC supplementation to support immune function to clear persistent human papillomavirus infections. Frontiers in Oncology. https://pubmed.ncbi.nlm.nih.gov/
- Gillison, M. L., et al. (2012). Prevalence of oral HPV infection in the United States, 2009–2010. JAMA, 307(7), 693–703.
- D'Souza, G., et al. (2007). Case-control study of human papillomavirus and oropharyngeal cancer. New England Journal of Medicine, 356(19), 1944–1956.
- Kreimer, A. R., et al. (2010). Oral human papillomavirus infection in adults is associated with sexual behavior and HIV serostatus. Journal of Infectious Diseases, 202(12), 1786–1792.
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







