


Receiving a test result that names HPV 16 or HPV 18 specifically is a different experience from a general HPV-positive result — and the fear that comes with it is understandable. These are high-risk strains, and that classification means something real. It also does not mean cancer is present, inevitable, or even likely. Most people who test positive for HPV 16 and HPV 18 clear the virus without ever developing cancer, and the process from initial infection to any serious cellular change takes many years — time that screening and proactive care are designed to use.
Key Takeaways
- HPV 16 and HPV 18 are high-risk strains, but a positive result is not a cancer diagnosis and should not be treated as one.
- Together, these two strains account for approximately 70% of cervical cancers globally — yet most people who carry them clear the infection naturally.
- Cancer from HPV 16 or 18 requires persistent, uncleared infection over many years, typically 10 to 20 years; it does not happen quickly.
- Regular screening, smoking cessation, and immune support are the most evidence-supported actions after a positive result.
- AHCC is the only supplement with a published, placebo-controlled human clinical trial specifically examining HPV clearance — though research is still preliminary.
In This Article
- What are HPV 16 and HPV 18?
- How common are they?
- Why are they considered high-risk?
- HPV 16 vs HPV 18 — are they different?
- Which cancers are linked to HPV 16 and 18?
- HPV 16 and 18 in women
- HPV 16 and 18 in men
- What does a positive result actually mean?
- What to do if you test positive
- Supporting immune clearance
- Frequently asked questions
What Are HPV 16 and HPV 18?
Human papillomavirus is a large family of more than 200 related viruses. Of these, approximately 14 are classified as high-risk types because of their association with cancer. HPV 16 and HPV 18 are two members of that high-risk group — and they are by far the most studied, most prevalent, and most commonly linked to HPV-attributable cancers worldwide.
All HPV strains infect epithelial cells — the cells that line skin and mucous membranes. What separates high-risk types from low-risk ones is not how they spread or how they feel (most HPV infections produce no symptoms at all), but what they are capable of doing inside infected cells over time. HPV 16 and HPV 18 carry genetic material that, under certain conditions, can interfere with the normal mechanisms cells use to regulate their own growth. This is what makes them worth monitoring — not because infection guarantees harm, but because persistent infection over many years creates a biological environment where abnormal cell changes become more likely.
It is also worth noting that HPV 16 and 18 are not uniquely dangerous in the sense that other high-risk strains (such as HPV 31, 33, 45, 52, and 58) also carry cancer risk. HPV 16 and 18 receive the most attention because they account for the largest share of HPV-related cancers and because current vaccines and genotyping tests are specifically designed to detect and protect against them.
How Common Are They?
HPV is the most common sexually transmitted infection in the United States. The CDC estimates that nearly all sexually active people will have HPV at some point in their lives, and that roughly 13 million new infections occur each year in the US alone. Within that broad picture, HPV 16 is the single most prevalent high-risk strain globally. HPV 18 is the second most common high-risk type.
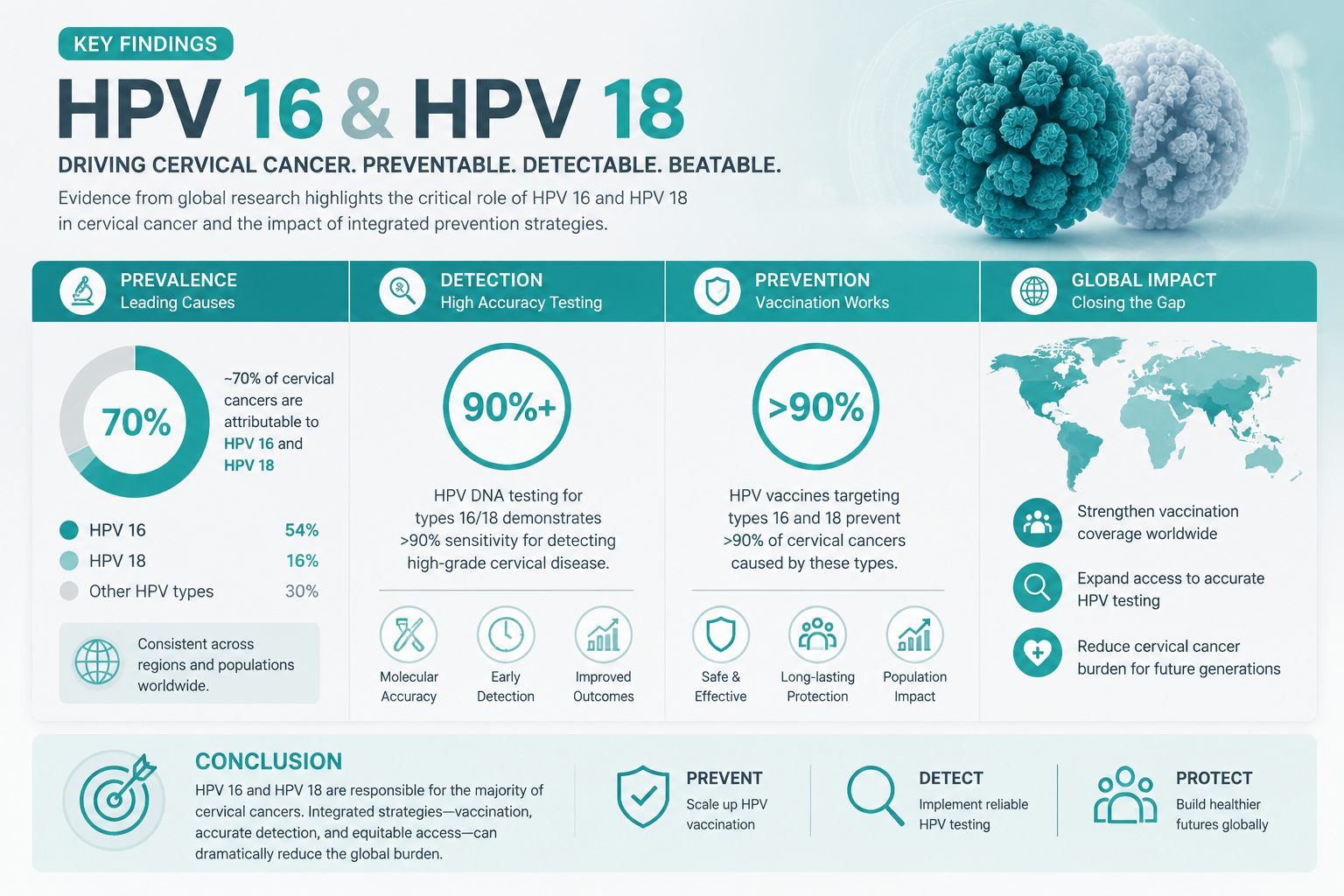
Together, HPV 16 and HPV 18 account for approximately 70% of all cervical cancers worldwide, according to the World Health Organization. That figure sounds alarming in isolation, but it needs context: the vast majority of people who carry these strains do not develop cervical cancer or any other HPV-related cancer. Clearance rates for HPV overall hover around 90% within two years of infection, and while high-risk strains like HPV 16 and 18 may take longer to clear than low-risk types, the immune system remains fully capable of resolving them in most people.
The risk is real and elevated compared to low-risk strains — that is precisely why genotyping tests exist. But prevalence and cancer risk are not the same thing. Millions of people carry HPV 16 or 18 at any given time, and the overwhelming majority will never develop cancer from it.
Why Are They Considered High-Risk?
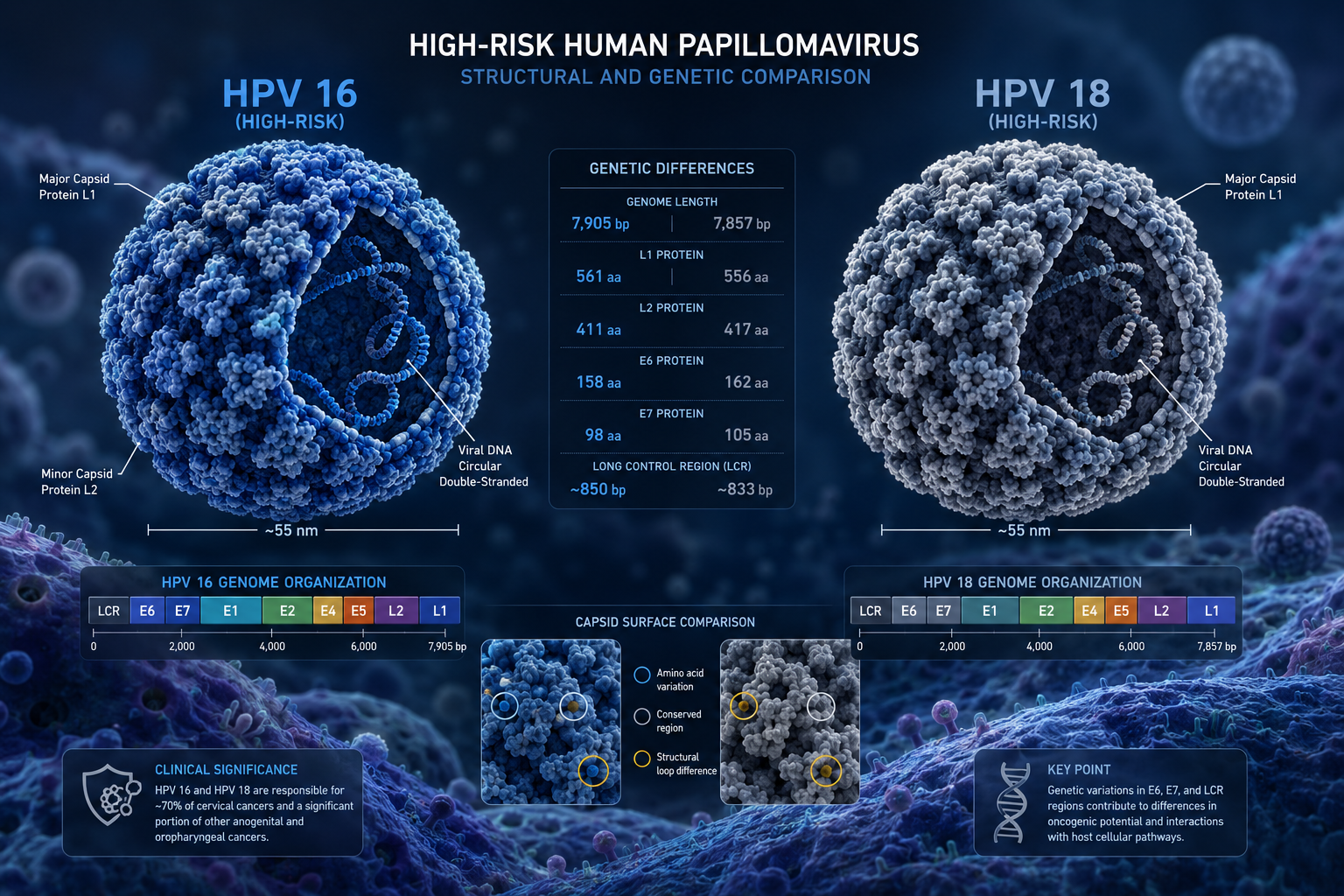
The "high-risk" label comes from a specific biological mechanism, not from how the virus feels or spreads. HPV 16 and HPV 18 produce two proteins — known as E6 and E7 oncoproteins — that are capable of disabling two of the body's most important tumor-suppressor proteins, called p53 and pRb. When these suppressor proteins are blocked, damaged or abnormal cells that would normally self-destruct can instead survive and continue dividing. Over many years of persistent infection, this creates conditions in which precancerous and eventually cancerous changes become possible.
This is a simplified summary of a complex biological process. For a full explanation of how HPV progresses from infection to cellular change, the article on how HPV causes cancer covers the mechanism in detail. The key point here is that this process is not instantaneous — it requires the virus to persist in the body without being cleared by the immune system, typically over a period of 10 to 20 years. A single positive test result does not mean that process has begun or that it will.
HPV 16 vs HPV 18 — Are They Different?
Both HPV 16 and HPV 18 are high-risk strains that share the same general mechanism of action, but they differ in meaningful ways — particularly in which cancers they are most associated with and how quickly they tend to progress.
| Feature | HPV 16 | HPV 18 |
|---|---|---|
| Primary cancer associations | Cervical, oropharyngeal, anal, penile | Cervical, vaginal, vulvar, adenocarcinoma |
| Share of cervical cancers | Approximately 55–60% | Approximately 10–15% |
| Cell type most affected | Squamous cells | Glandular cells (adenocarcinoma) |
| Persistence tendency | Higher | Moderate |
| Progression timeline | Generally slower, more time for screening to catch changes | Can progress more quickly to glandular lesions |
| Detection on standard Pap smear | Reliable | Slightly less reliable for glandular changes |
One clinically important distinction: HPV 18 has a stronger association with adenocarcinoma — a cancer that originates in glandular cells rather than the squamous cells that line the surface of the cervix. Glandular lesions can be harder to detect on a standard Pap smear, which is one reason that an HPV 18-positive result may prompt earlier or more thorough follow-up, even when a Pap smear appears normal. If you have received a result showing HPV 18 with a normal Pap, the article on HPV positive but normal Pap results explains what that combination means and what follow-up typically looks like.
Both strains are covered by current genotyping tests, and both are targeted by the HPV vaccines currently available.
Which Cancers Are Linked to HPV 16 and 18?
HPV 16 and HPV 18 together are associated with a range of cancers beyond the cervix. The National Cancer Institute provides attribution estimates for HPV across cancer types. The table below summarizes the approximate combined contribution of HPV 16 and 18:
| Cancer Type | Approximate HPV 16 + 18 Attribution |
|---|---|
| Cervical | ~70% |
| Oropharyngeal (throat/tonsil) | ~60–70% |
| Anal | ~80–90% |
| Vaginal | ~55–65% |
| Vulvar | ~30–40% |
| Penile | ~45–55% |
These figures represent the proportion of each cancer type that is attributable to HPV 16 and 18 specifically — they are not individual risk percentages. Oropharyngeal cancers (cancers of the throat, tonsils, and base of the tongue) are a growing area of concern, particularly in men, and HPV 16 is the dominant driver in that category. The article on oral HPV infection covers the oropharyngeal context in full, including how oral HPV is acquired and what monitoring options exist.
The cancer risk associated with HPV 16 and 18 is real and worth taking seriously. It is also worth keeping in perspective: these attribution percentages describe what proportion of existing cancers involve these strains — not the probability that any individual with a positive test will develop cancer.
HPV 16 and 18 in Women
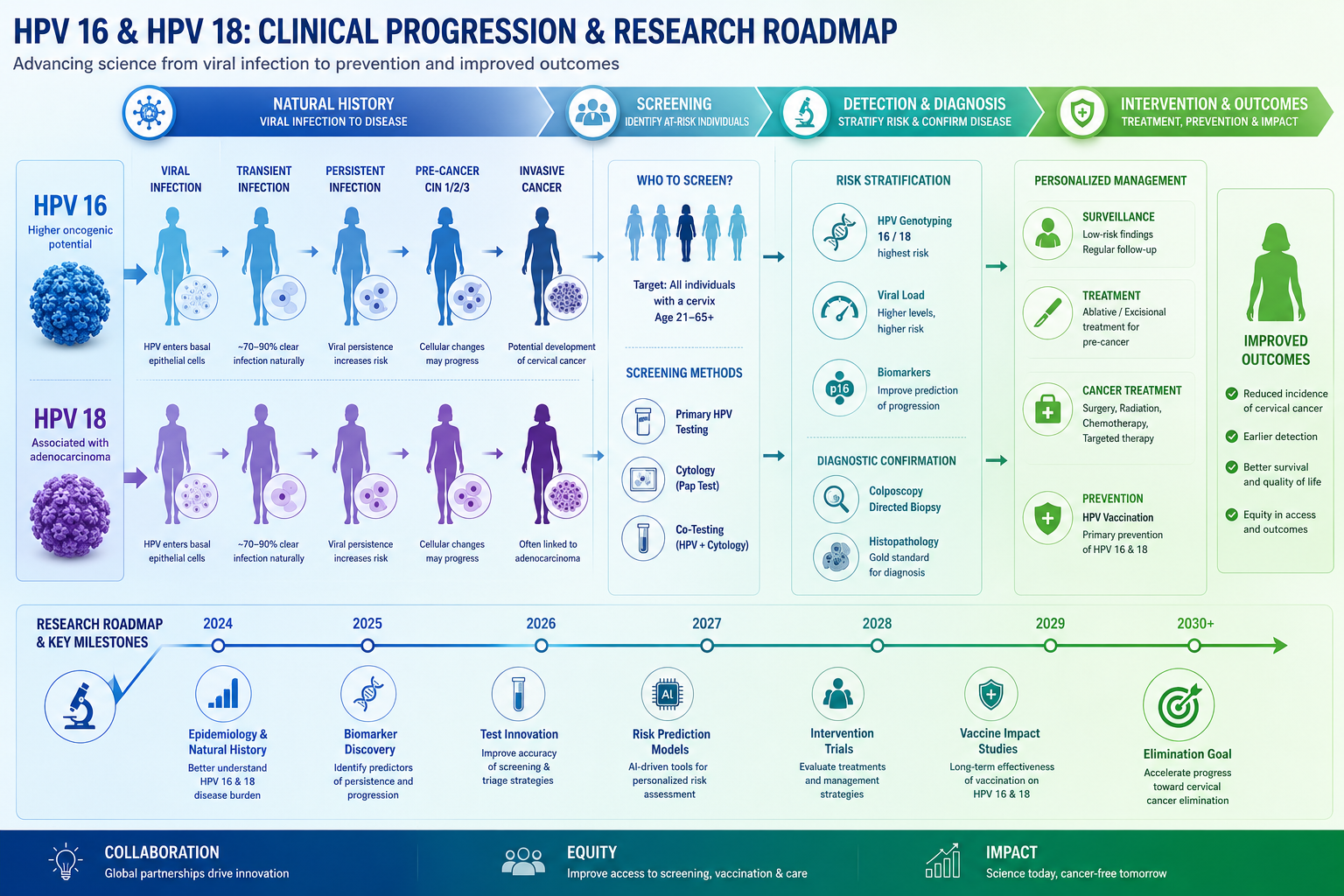
Women have a significant structural advantage when it comes to HPV 16 and 18: routine cervical screening. Pap smears and HPV co-testing are specifically designed to catch the cellular changes that these strains can cause — long before those changes become cancer. This is not a coincidence; the entire cervical screening system was built around the biology of HPV-related cervical cancer, which progresses slowly enough that regular monitoring can interrupt it at a precancerous stage.
When a woman tests positive for HPV 16 or 18, the typical clinical response is enhanced monitoring rather than immediate treatment. This usually means a colposcopy — a closer examination of the cervix — and more frequent follow-up testing. If precancerous changes (called cervical intraepithelial neoplasia, or CIN) are found, they are classified by grade and monitored or treated accordingly. CIN findings are not cancer. They are cellular changes that exist on a spectrum, many of which resolve on their own, particularly at lower grades.
The existence of this screening pathway is genuinely reassuring. A positive HPV 16 or 18 result in a woman who is engaged with regular screening is a finding that the system is designed to manage. The risk is elevated compared to low-risk strains, but it is a risk being actively watched — which is a very different situation from an undetected, unmonitored infection.
HPV 16 and 18 in Men
Men face a different challenge with HPV 16 and 18: there is currently no routine, approved screening test for HPV in men equivalent to the cervical Pap smear. This means that most men carry HPV 16 or 18 without knowing it, and the infection either clears on its own or — in a smaller subset — persists and contributes to cancer development over many years.
HPV 16 is the primary driver of oropharyngeal cancer in men, a cancer type that has been rising in incidence over recent decades. It is also associated with anal and penile cancers, though these are less common. Men who have received a partner's HPV 16 or 18 diagnosis, who have specific risk factors (such as a history of anal intercourse or immune suppression), or who have noticed symptoms should raise these concerns with their healthcare provider to discuss whether any monitoring options are appropriate for their situation.
For a comprehensive look at HPV in men — including why symptoms are rare, what the actual risk profile looks like, and what options exist — the article on HPV in men covers this topic in full.
What Does a Positive Result Actually Mean?
A positive result for HPV 16 or HPV 18 means one specific thing: the virus was detectable in the tissue sample that was tested at the time of the test. It does not mean cancer is present. It does not mean cancer is certain. It does not mean the infection will not clear. These are not reassuring platitudes — they are accurate statements about what the test result actually tells you.
Here is what the evidence actually shows. Most people who test positive for high-risk HPV, including HPV 16 and 18, will clear the infection without developing cancer. The immune system is the primary mechanism for HPV clearance, and it is effective in the large majority of cases. The risk with HPV 16 and 18 is that they are more likely than low-risk strains to persist — and it is persistent, long-term infection that creates the conditions for cancer, not a single positive test.
The timeline matters enormously here. The progression from initial HPV infection to cervical cancer, when it does occur, typically takes 10 to 20 years. That is not a timeline that makes a positive test result an emergency. It is a timeline that makes regular monitoring, immune health, and lifestyle choices genuinely meaningful — because there is time for the immune system to act, and time for screening to catch any changes early.
What a positive result does mean, practically speaking, is that closer monitoring is warranted, and that taking steps to support immune function is a reasonable and evidence-informed response. It is a finding to act on — not a sentence to fear.
What to Do If You Test Positive
A positive result for HPV 16 or 18 calls for a clear, calm response. The following steps reflect current clinical guidance and evidence-based lifestyle recommendations.
1. Follow your provider's monitoring schedule without delay. If your provider recommends a colposcopy, repeat HPV testing, or more frequent Pap smears, follow through on that schedule. Monitoring is not passive — it is the active clinical tool that catches changes early, when they are most manageable.
2. Stop smoking if you currently smoke. This is the single most impactful lifestyle change for HPV persistence. Smoking suppresses local immune function in cervical tissue and is strongly associated with slower HPV clearance and higher rates of progression to precancerous changes. The evidence on this point is consistent and substantial.
3. Address nutritional deficiencies, particularly vitamin D and folate. Low vitamin D levels are associated with impaired immune function broadly, and research from the NIH supports the role of adequate vitamin D in immune regulation. Folate deficiency has been linked to increased susceptibility to HPV-related cervical changes. A blood test can identify deficiencies that are worth correcting.
4. Prioritize sleep and stress management. Chronic sleep deprivation and elevated cortisol from ongoing stress both suppress immune function. These are not minor lifestyle factors — they have measurable effects on the immune system's ability to identify and respond to viral infections, including HPV.
5. Discuss evidence-based supplement options with your provider. If you want to explore additional immune support, AHCC is the supplement with the most relevant published clinical research for HPV specifically. Understanding why HPV doesn't clear in some people can also help you identify factors in your own situation that may be worth addressing.
Supporting Immune Clearance
The immune system is the only mechanism that clears HPV 16 and HPV 18. No antiviral medication currently targets HPV directly. This makes immune health not just a general wellness recommendation but a clinically relevant priority for anyone managing a high-risk HPV infection.
The lifestyle factors with the strongest evidence behind them are smoking cessation (discussed above), adequate sleep (7 to 9 hours for most adults), stress reduction, and correcting nutritional deficiencies in vitamin D and folate. These are not small interventions — each one has a measurable effect on immune function, and together they create conditions in which the immune system is better positioned to do what it is already trying to do.
On the supplement side, AHCC (Active Hexose Correlated Compound) is a standardized extract derived from hybridized medicinal mushroom mycelia. It is the only supplement with a published, placebo-controlled human clinical trial specifically examining HPV clearance. That trial, conducted by Dr. Judith Smith at the University of Texas Health Science Center at Houston, used 3 grams per day taken on an empty stomach for a minimum of six months. The results were promising. This research is preliminary — it has not been replicated at scale, and AHCC is not FDA-approved as an HPV treatment — but it represents a meaningful starting point that no other supplement in this category can match. For a thorough review of what that research actually shows, the article on whether AHCC really helps clear HPV covers the clinical evidence in full detail.
For those who want to explore AHCC as part of a broader immune support strategy, NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility. At the research-validated dose of 3 grams per day, that equates to approximately four to five capsules daily, taken on an empty stomach. For specific dosage guidance, the article on what dosage of AHCC to take for HPV outlines what the clinical studies used and how to apply that to a practical protocol.
Frequently Asked Questions
Does HPV 16 or 18 always cause cancer?
No. The large majority of people who test positive for HPV 16 or HPV 18 will not develop cancer. Cancer from these strains requires persistent, long-term infection — typically over 10 to 20 years — during which the virus continuously evades immune clearance and drives progressive cellular changes. Most infections, including those caused by high-risk strains, are resolved by the immune system before reaching that stage. Regular screening and proactive immune support are the tools that make a positive outcome more likely.
Can HPV 16 or 18 clear on its own?
Yes. The immune system is capable of clearing HPV 16 and HPV 18, just as it clears other HPV strains. Clearance may take longer with high-risk types than with low-risk ones — sometimes up to two years or more — but it does occur in the majority of cases. Factors that support clearance include non-smoking status, healthy immune function, adequate sleep, and good nutritional status. A positive result at one test does not guarantee a positive result at the next.
What is the difference between HPV 16 and HPV 18?
Both are high-risk strains that share the same general mechanism, but they differ in their cancer associations and the cell types they most commonly affect. HPV 16 is more strongly linked to squamous cell cancers, including cervical, oropharyngeal, anal, and penile cancers, and accounts for the larger share of cervical cancers (approximately 55–60%). HPV 18 is more associated with glandular cell cancers (adenocarcinoma) and accounts for roughly 10–15% of cervical cancers. HPV 18-related lesions can sometimes be harder to detect on a standard Pap smear, which may influence the follow-up approach your provider recommends.
Should I be tested for HPV 16 and 18 specifically?
Genotyping tests that identify HPV 16 and 18 specifically are available and are often included in extended HPV testing panels. Whether you need one depends on your age, screening history, and prior results. Current guidelines from major medical organizations recommend HPV co-testing (Pap plus HPV test) for women aged 30 and older, and genotyping for HPV 16 and 18 is often performed when an HPV-positive result is found. Your healthcare provider is the right person to determine whether genotyping is appropriate for your situation.
What is the next step after testing positive for HPV 16 or 18?
The most important next step is to follow the monitoring plan your healthcare provider recommends — whether that is a colposcopy, more frequent Pap testing, or repeat HPV testing at a set interval. Beyond that, the evidence-supported actions are stopping smoking (if applicable), addressing vitamin D and folate deficiencies, prioritizing sleep and stress management, and discussing whether immune support supplements like AHCC are appropriate for your situation. A positive result is a prompt to act thoughtfully — not a reason to panic.
Conclusion
HPV 16 and HPV 18 are the two most studied and most consequential high-risk strains in the HPV family. A positive result for either one deserves attention, follow-through, and honest conversation with a healthcare provider. It does not deserve fear that outpaces the actual evidence.
The biology of these strains is well understood: they carry a higher risk of persistence and cellular disruption than low-risk types, and persistent infection over many years can — in a minority of cases — lead to cancer. That risk is real. It is also manageable, particularly when it is caught through screening and met with consistent immune support and healthy lifestyle choices.
Concrete next steps:
- Schedule or confirm your follow-up appointment — colposcopy, repeat testing, or whatever your provider has recommended — and keep it.
- Stop smoking if you currently smoke. No other single action has stronger evidence for reducing HPV persistence and progression.
- Get a blood test to check vitamin D and folate levels, and address any deficiencies with your provider's guidance.
- Prioritize sleep (7 to 9 hours), reduce chronic stress where possible, and treat immune health as the clinical priority it is.
- Ask your provider about AHCC if you want to explore evidence-based supplement support — and use that conversation to make an informed, personalized decision.
Related Reading
- Understand the biological pathway from HPV infection to cellular change in the article on how HPV causes cancer.
- If your Pap smear was normal but your HPV result was positive, the article on HPV positive with a normal Pap explains what that combination means and what to expect next.
- For a thorough review of the clinical evidence behind AHCC for HPV, see does AHCC really help clear HPV.
- If you are wondering why some infections clear quickly while others persist, why HPV doesn't clear in some people covers the key factors in detail.
References
- Centers for Disease Control and Prevention. Human Papillomavirus (HPV). https://www.cdc.gov/hpv
- World Health Organization. Human papillomavirus (HPV) and cervical cancer. Fact sheet. 2023. https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer
- National Cancer Institute. HPV and Cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
- National Institutes of Health, Office of Dietary Supplements. Vitamin D: Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
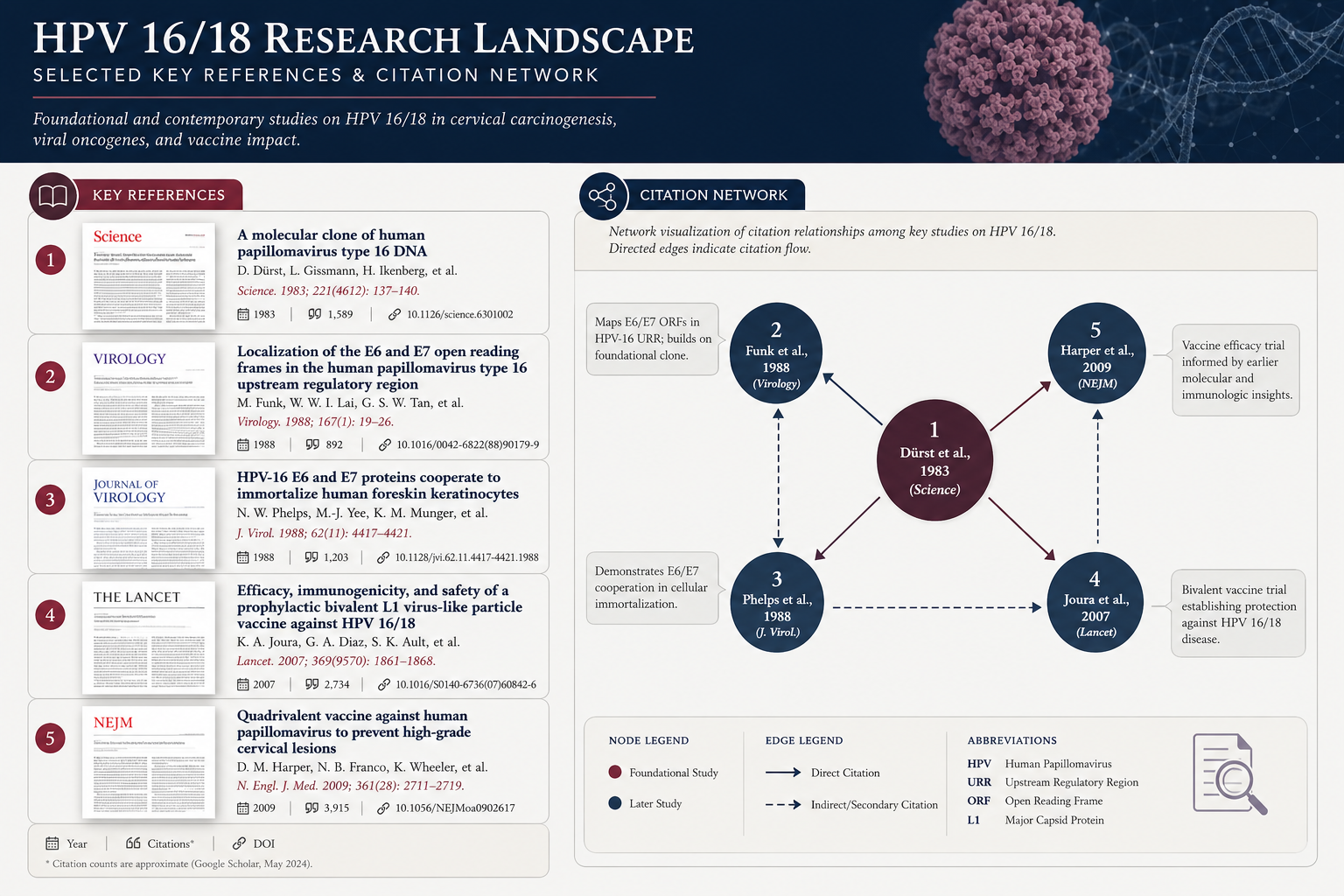
- Smith JA, et al. "Medicinal Mushroom Extracts and Human Papillomavirus (HPV): A Pilot Study." Published research available via PubMed. https://pubmed.ncbi.nlm.nih.gov/
- Bosch FX, et al. "Epidemiology and Natural History of Human Papillomavirus Infections and Type-Specific Implications in Cervical Neoplasia." Vaccine. 2008.
- de Sanjose S, et al. "Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study." Lancet Oncology. 2010.
- Schiffman M, et al. "Human papillomavirus and cervical cancer." Lancet. 2007.
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







