


According to the CDC, human papillomavirus is the most common sexually transmitted infection in the United States, yet no antiviral treatment exists to clear it — the immune system must do that work. That gap is precisely why AHCC dosage for HPV has become one of the most searched supplement questions in integrative medicine. Most sources tell you the answer — 3 grams per day, fasted, for 6 months — but few explain where that number comes from, what the research actually tested, and what the evidence says about taking more or less. This article addresses those questions directly, from the published clinical record.
Key Takeaways
- The 3-gram daily AHCC dose for HPV comes from a specific published Phase II randomized, double-blind, placebo-controlled clinical trial led by Dr. Judith Smith at the University of Texas Health Science Center at Houston — not from supplement marketing.
- The trial tested one dose (3 grams) against placebo; it did not compare multiple dose levels, so there is no published evidence that lower doses produce HPV clearance.
- Doses of 500mg to 1 gram per day are standard for general immune support but fall below the HPV-specific research protocol.
- The 6-month duration is the trial's primary assessment point — not an arbitrary minimum.
- AHCC is not FDA-approved to treat HPV; this is one Phase II trial, and replication in larger studies is needed before clinical guidelines change.
In This Article
- The clinical trial that established the protocol
- Why 3 grams — where that number comes from
- What the trial actually found
- What happens at lower doses
- What about higher doses?
- The 6-month duration — what the research shows
- The empty-stomach protocol — the evidence behind it
- AHCC dosing in other clinical contexts
- What this means for your protocol
- Frequently asked questions
The 3-gram daily AHCC protocol for HPV is not a general supplement recommendation — it comes from a specific published clinical trial design.
The Clinical Trial That Established the Protocol
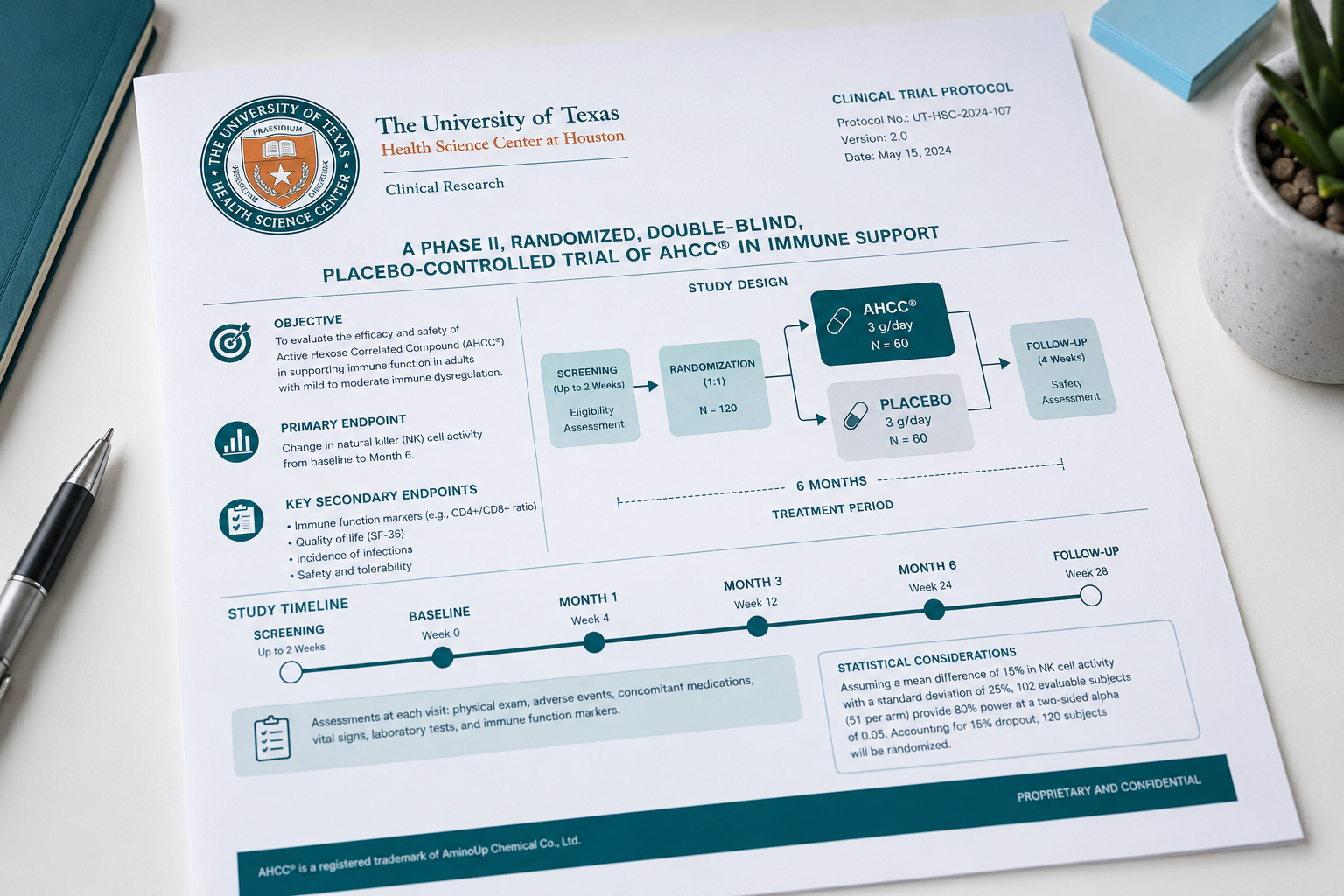
The 3-gram AHCC dosage for HPV has a single, traceable origin: a Phase II randomized, double-blind, placebo-controlled trial led by Dr. Judith Smith at the University of Texas Health Science Center at Houston. This is the primary — and, to date, only — published human clinical trial specifically designed to evaluate AHCC for HPV clearance. Understanding the trial design is essential to understanding why the protocol is what it is.
Trial design at a glance:
| Element | Detail |
|---|---|
| Study type | Randomized, double-blind, placebo-controlled Phase II trial |
| Population | Women with persistent high-risk HPV infections |
| Intervention | AHCC at 3 grams per day, taken fasted |
| Comparator | Placebo |
| Duration | 6 months of active supplementation |
| Primary endpoint | HPV clearance status at 6 months |
| Follow-up | Clearance status assessed after AHCC discontinuation |
Every element of the protocol that practitioners now recommend — the dose, the fasted timing, the 6-month minimum — is drawn directly from this trial design. When a clinician recommends 3 grams on an empty stomach for 6 months, they are recommending the protocol that was tested in a controlled setting, not a dose chosen by intuition or convention.
The published research is indexed on PubMed and represents the foundation of the current evidence base for AHCC and HPV. No other controlled human trial has been published that specifically tests AHCC for HPV clearance at any dose.
Dr. Judith Smith's Phase II trial at the University of Texas Health Science Center at Houston is the primary published human evidence for AHCC and HPV.
Why 3 Grams — Where That Number Comes From
The 3-gram dose was not selected randomly. Before the HPV-specific trial was designed, AHCC had been studied across multiple immune function and oncology contexts. Research on AHCC's immune-modulating effects — particularly on natural killer (NK) cell activity and cytokine production — suggested that 3 grams represented a dose at which clinically meaningful immune modulation could be observed in adult populations. For a broader look at how AHCC interacts with immune function, the NIH's overview of immune system research provides useful foundational context.
A critical distinction that is often missed: the dose-response relationship for AHCC's effects on HPV clearance specifically has not been studied in a controlled trial. The Smith et al. trial tested 3 grams — it did not test 1 gram, 2 grams, or 4 grams as separate arms. What the published evidence shows is that 3 grams produced statistically significant results compared to placebo. What it does not show is whether a different dose would produce the same, greater, or lesser effect.
For readers curious about the biological mechanism by which AHCC may support the immune system's response to HPV, how AHCC clears HPV covers that topic in depth. The short version: AHCC appears to support immune surveillance through NK cell and dendritic cell activity — and 3 grams is the dose at which this modulation has been most consistently observed across published research.
The practical implication is direct: replicating the trial protocol exactly — rather than adjusting the dose based on cost, convenience, or intuition — is the most defensible approach for anyone using AHCC specifically for HPV. Deviating from the researched protocol means operating outside the evidence base.
What the Trial Actually Found
The trial found statistically significant HPV clearance in the AHCC group compared to placebo at the 6-month assessment point. In participants who cleared HPV during the active supplementation period, clearance was sustained at follow-up testing after AHCC was discontinued — a finding that suggests the immune response, once established, may persist beyond the supplementation period. Not every participant cleared HPV; AHCC does not produce universal results, and this is one Phase II trial requiring replication in larger studies before clinical guidelines change.
For a complete breakdown of the trial design, results, limitations, and what the data actually support, see does AHCC really help clear HPV — that article covers the evidence in full detail without the scope constraints of this one.
What Happens at Lower Doses
This is one of the most practically important questions in the AHCC and HPV conversation, and the answer from the published literature is straightforward: there is no published evidence that doses below 3 grams per day produce HPV clearance.
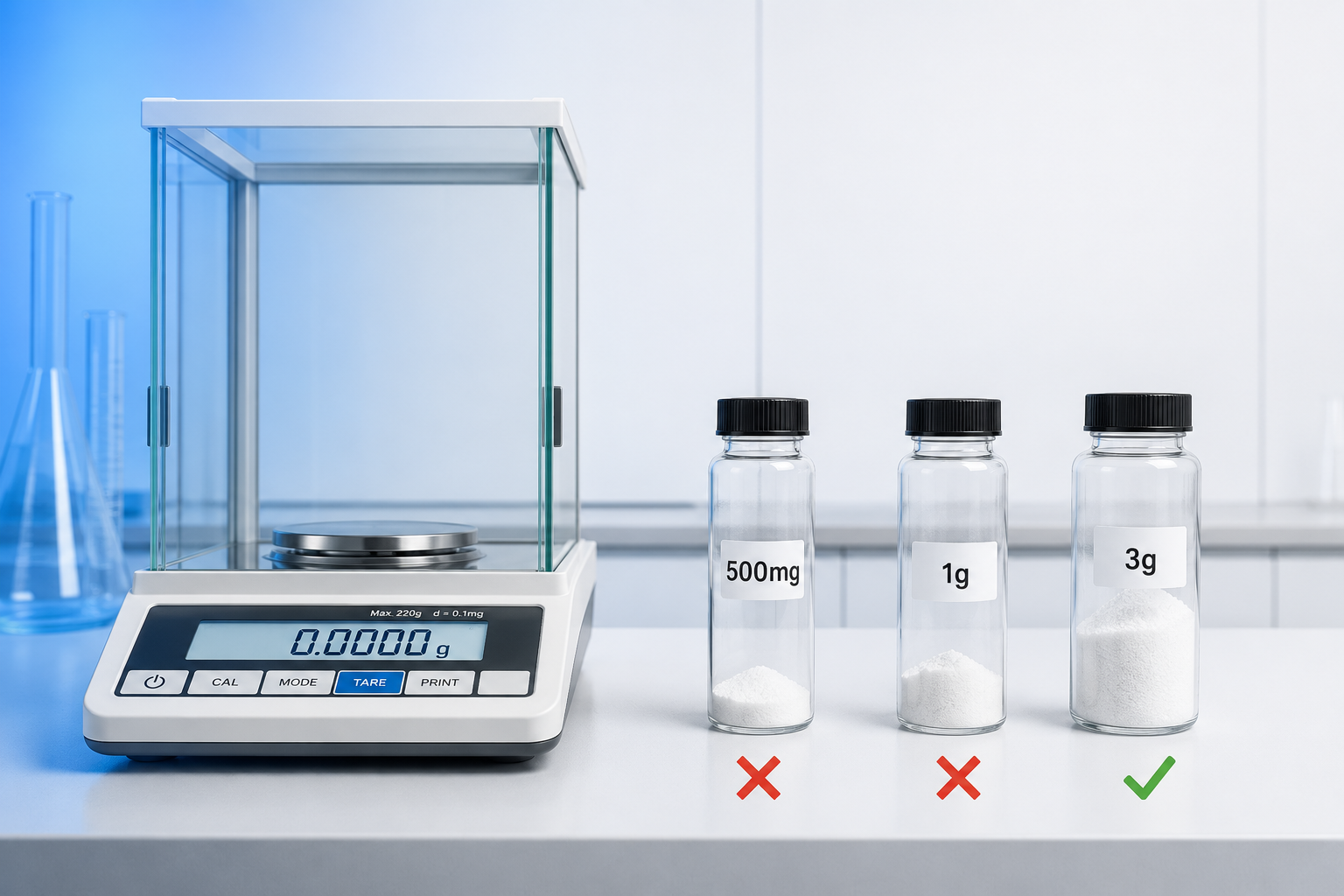
Most AHCC products on the market are positioned for general immune support at doses of 500mg to 1 gram per day. This is the standard wellness dose — appropriate for general immune maintenance, but not the HPV-specific research protocol. The distinction matters enormously for anyone taking AHCC specifically to support HPV clearance.
| Dose Range | Evidence Level | Context |
|---|---|---|
| 500mg–1g/day | General immune support use | Standard wellness dose; not studied for HPV clearance |
| 1g–2g/day | No HPV-specific evidence | Below the researched protocol; no controlled data |
| 3g/day | Published Phase II trial | Only dose with HPV-specific human clinical data |
| Above 3g/day | No additional benefit established | Higher doses not supported by HPV-specific evidence |
The gap between the general wellness dose and the HPV research dose is significant — a person taking one 500mg capsule per day is receiving one-sixth of the dose used in the published trial. Extrapolating that this would produce similar HPV outcomes is not supported by any published evidence.
Lower doses are commonly used for general immune maintenance but fall below the dose studied in published HPV-specific research.
For people who have been taking AHCC at lower doses and are not seeing results, underdosing is one of the most common and most correctable protocol errors. A thorough analysis of why AHCC protocols fail — including dose, timing, and product quality issues — is covered in the real reasons AHCC didn't work for you.
What About Higher Doses?
Patients sometimes ask whether taking more than 3 grams per day might produce faster or more reliable results. The honest answer from the published evidence: there is no clinical data showing that doses above 3 grams per day produce better HPV outcomes. No HPV-specific trial has tested higher doses, and there is no dose-escalation study in the HPV context to draw from.
In oncology and liver health contexts, AHCC has been used at higher doses under direct clinical supervision — but these are different indications, different patient populations, and different clinical goals. The evidence from those contexts does not transfer directly to HPV clearance.
AHCC has a well-documented safety profile, and higher doses have not demonstrated significant toxicity in published research. However, the absence of harm is not the same as evidence of benefit. There is no published clinical rationale for exceeding 3 grams per day specifically for HPV, and doing so increases cost and adherence burden without a supporting evidence base. More is not necessarily more when the dose-response curve for the specific outcome has not been studied.
The 6-Month Duration — What the Research Shows
The 6-month minimum duration is not a conservative estimate or a marketing convention — it is the trial's primary assessment point. The Smith et al. trial measured HPV clearance at 6 months. That is when the primary endpoint was evaluated, and that is the timeframe within which statistically significant clearance was observed in the AHCC group.
Testing at 3 months and concluding the protocol has failed is not consistent with how the evidence was generated. Participants who showed clearance at 6 months may not have shown it at 3 months — the immune response to HPV takes time to develop and consolidate, and the trial was designed with that biology in mind.
Some practitioners extend the protocol to 9 to 12 months for high-risk strains — particularly HPV 16 — or for individuals managing multiple concurrent infections. This is reasonable clinical practice, but it goes beyond the published protocol; no controlled trial has specifically evaluated extended duration. For a detailed look at what the research and clinical experience suggest about timing, see how long does AHCC take to clear HPV.
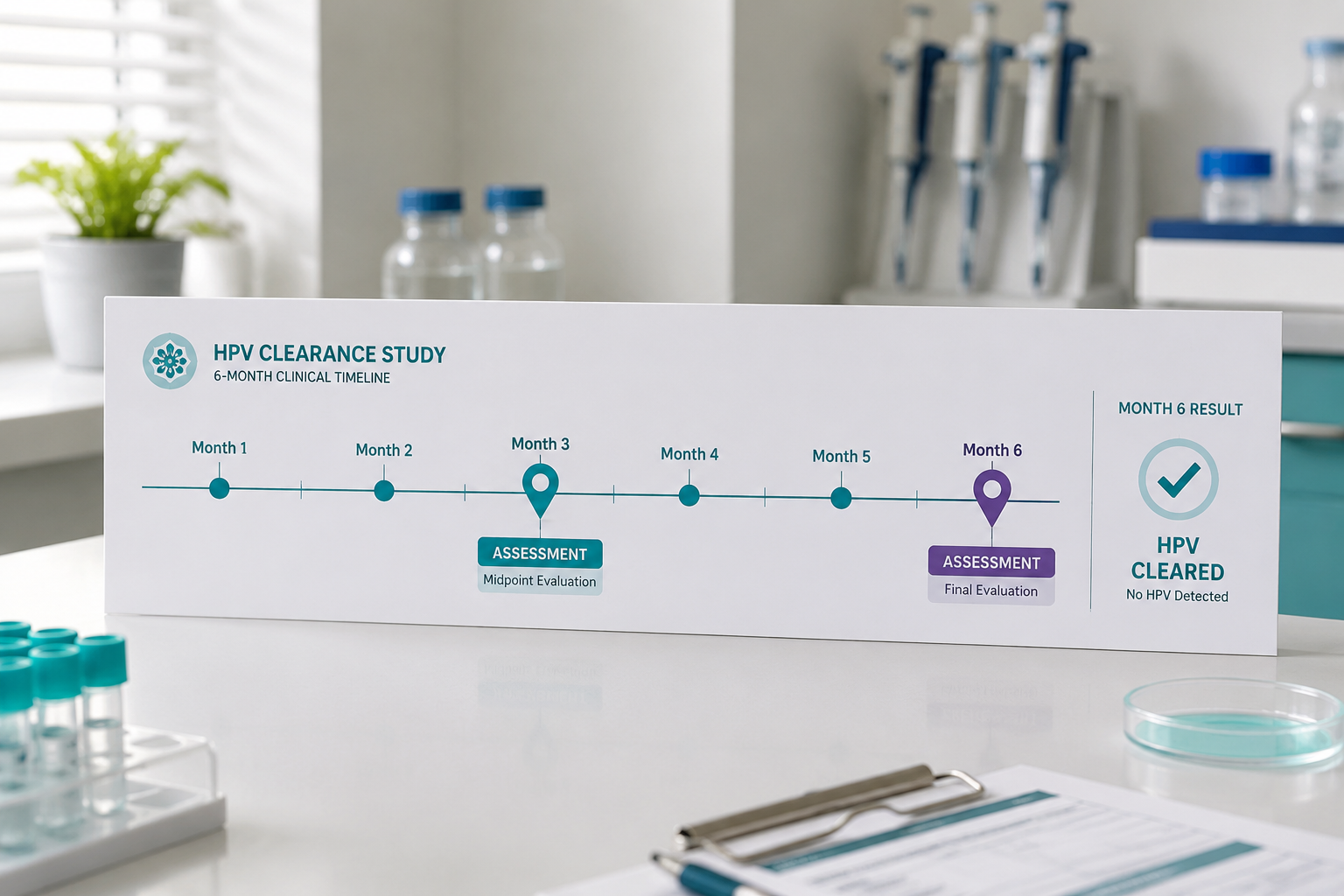
The trial assessed HPV status at 6 months — this is why the protocol is a minimum of 6 months, not an arbitrary recommendation.
The Empty-Stomach Protocol — The Evidence Behind It
The trial protocol specified fasted dosing, and this detail is part of the published methodology — not an add-on recommendation. The rationale rests on general principles of polysaccharide absorption: fasted conditions allow faster gastric emptying and potentially more efficient uptake of AHCC's alpha-glucan fraction in the small intestine. Food — particularly fat and protein — slows gastric emptying and may reduce absorption efficiency for compounds like AHCC.
One important caveat deserves acknowledgment: AHCC's absorption kinetics have not been studied in a dedicated fasted-versus-fed pharmacokinetic trial. The empty-stomach protocol reflects the trial design and is supported by general absorption principles — not by AHCC-specific bioavailability data comparing the two conditions directly.
For the full explanation of why fasted dosing is recommended, how long before eating AHCC should be taken, and what to do if fasted dosing causes discomfort, see why take AHCC on an empty stomach.
AHCC Dosing in Other Clinical Contexts
AHCC has been studied across a range of clinical applications beyond HPV, and examining those contexts provides useful perspective on why 3 grams was selected as the HPV trial dose. The broader AHCC clinical research indexed on PubMed spans oncology, liver health, influenza prevention, and general immune support.
| Clinical Context | Dose Used in Research | Notes |
|---|---|---|
| General immune support | 500mg–1g/day | Standard wellness use; widely available |
| Cancer adjunct therapy | 3g/day | Multiple published studies; different indication |
| Liver health | 3g/day | Japanese clinical use; published data |
| Influenza prevention | 3g/day | Small published trials |
| HPV clearance | 3g/day | One Phase II trial (Smith et al.) |
The consistency of 3 grams per day across multiple immune and clinical applications is not coincidental. It reflects a pattern in the AHCC research literature: 3 grams appears to be the dose at which AHCC produces clinically meaningful immune modulation across studied contexts. This cross-context consistency provided the scientific rationale for selecting 3 grams as the dose for the HPV trial — it was the dose with the strongest existing immune-modulation evidence base.
What This Means for Your Protocol
The published evidence supports one specific protocol: 3 grams of AHCC per day, taken fasted, for a minimum of 6 months. This is not a general immune support dose — it is the HPV-specific research protocol, and every element of it reflects a deliberate choice made in the trial design.
Every deviation from this protocol — lower dose, shorter duration, taking with food — reduces fidelity to the evidence base that produced the published results. That does not mean deviations are dangerous; it means they move the protocol further from what was actually studied.
NovaHerbs AHCC provides 700mg per capsule, manufactured in a GMP-certified facility in the USA. At 3 grams per day, that is approximately 4 to 5 capsules taken together once daily on an empty stomach — a straightforward protocol that aligns with the published trial methodology.

NovaHerbs AHCC provides 700mg per capsule — at 3 grams per day, that is approximately 4–5 capsules taken together on an empty stomach.
For full practical guidance on structuring the daily protocol — including timing, what to do if you miss a dose, and how to track progress — see what dosage of AHCC should I take for HPV. That article covers practical implementation in full detail. This article's purpose is the evidence behind the protocol. Now you have both.
Frequently Asked Questions
Why exactly 3 grams and not 2 or 4?
The 3-gram dose was selected for the HPV trial based on prior AHCC research showing clinically meaningful immune modulation at that dose level in adult populations. The trial did not test 2 grams or 4 grams as separate arms, so there is no published comparison data. What the evidence shows is that 3 grams produced statistically significant results compared to placebo. Choosing a different dose — lower or higher — means operating without HPV-specific clinical data to support that choice. Until a dose-comparison trial is published, 3 grams remains the only dose with direct HPV-specific human evidence.
Is the 3-gram dose safe?
AHCC has a well-documented safety profile across multiple published studies and decades of clinical use in Japan and internationally. At 3 grams per day, adverse effects reported in the published literature have been mild and infrequent, typically limited to minor gastrointestinal symptoms in some individuals. AHCC is generally considered well-tolerated at the researched dose. That said, individuals with specific health conditions, those taking immunosuppressive medications, or those who are pregnant or breastfeeding should consult a healthcare provider before beginning any supplement regimen. AHCC is a supplement, not a pharmaceutical, and individual responses vary.
Did the clinical trial test different AHCC doses?
No. The Smith et al. Phase II trial tested one dose: 3 grams per day. It was designed as a proof-of-concept trial to establish whether AHCC at the researched immune-modulation dose could produce HPV clearance compared to placebo — not as a dose-finding study. A dose-finding study would test multiple dose levels simultaneously to identify the optimal range. That study has not been published for HPV specifically. This is an important limitation of the current evidence base, and it is one reason why replicating the trial protocol exactly is the most defensible approach.
What happens if I cannot afford 3 grams per day — is a lower dose better than nothing?
This is a reasonable and honest question. The truthful answer is that there is no published evidence showing that lower doses produce HPV clearance, so a lower dose cannot be recommended as an equivalent alternative based on the current research. Whether a lower dose provides any partial benefit for HPV is unknown — the trial did not test it. If cost is a barrier to the full 3-gram protocol, that conversation is worth having with a healthcare provider who can help weigh options. Choosing a high-quality AHCC product with verified potency is also essential — a lower-cost product at the correct dose is preferable to an unverified product at any dose.
Was the AHCC trial only done in women?
The published Phase II trial enrolled women with persistent high-risk HPV infections. This reflects the clinical context in which HPV-related disease is most commonly monitored and diagnosed — through cervical screening programs. The trial was not designed to exclude men; it was designed around the population in which HPV persistence and clearance can be most directly measured through established clinical endpoints. Whether the results apply equally to men has not been studied in a controlled trial. AHCC's immune-modulating mechanisms are not sex-specific in the broader research literature, but HPV-specific evidence in male populations remains an open research question.
Conclusion
The AHCC dosage for HPV that practitioners recommend — 3 grams per day, fasted, for 6 months — is not a general supplement guideline. It is a research protocol drawn from a specific published clinical trial, and every element of it reflects a deliberate methodological choice. Understanding where the dose comes from, why it was selected, and what the evidence does and does not support is the foundation of an informed decision.
Actionable next steps:
- Verify your dose. If you are currently taking AHCC at less than 3 grams per day for HPV support, review your protocol against the published trial dose. Underdosing is the most common correctable protocol error.
- Commit to the full duration. The 6-month minimum is the trial's primary assessment point — not a suggestion. Evaluating results before 6 months is not consistent with how the evidence was generated.
- Follow the fasted protocol. Take AHCC on an empty stomach as specified in the trial methodology. This is a protocol detail, not a preference.
- Consult your healthcare provider. AHCC is a supplement, not a treatment. Bring the published research to your provider, continue recommended HPV monitoring, and make decisions within a supervised care context.
Related Reading
- Does AHCC really help clear HPV? What the research actually says
- What dosage of AHCC should I take for HPV? Practical implementation guide
- How long does AHCC take to clear HPV?
- The real reasons AHCC didn't work for you
- Why take AHCC on an empty stomach? The science behind timing your supplement
References
- Smith JA et al. AHCC supplementation to support immune function to clear persistent HPV infections. Available on PubMed.
- Centers for Disease Control and Prevention. HPV fact sheet. https://www.cdc.gov/hpv
- National Institute of Allergy and Infectious Diseases. Immune system overview. https://www.niaid.nih.gov/research/immune-system
- PubMed — AHCC broader clinical research (oncology and immune contexts). https://pubmed.ncbi.nlm.nih.gov/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







