


Roughly 1 in 10 school-age children will develop a common wart at some point — and every single one of those warts is an HPV infection. For most parents, the word "HPV" triggers immediate alarm because of its association with sexually transmitted infections and cervical cancer. That association, while real in adult contexts, tells almost none of the story when it comes to HPV in children. The overwhelming majority of pediatric HPV infections are harmless skin warts with no health consequences, and most resolve on their own without any treatment. Understanding what HPV actually looks like in children — and when it genuinely requires medical attention — changes the conversation from panic to informed action.
Key Takeaways
- Most HPV in children refers to common skin warts — medically harmless and extremely prevalent in school-age children.
- Genital HPV in a prepubescent child can occur through non-sexual routes, but always requires evaluation by a trained healthcare provider.
- HPV-related cancer in children is extremely rare; cancer requires persistent high-risk infection over many years.
- The HPV vaccine is recommended at ages 11–12 and is one of the most effective cancer prevention tools available for both boys and girls.
- Children's immune systems typically clear HPV faster than adult immune systems — most warts resolve spontaneously within one to two years.
In This Article
- Types of HPV most common in children
- How children get HPV
- Symptoms in children and adolescents
- Genital HPV in children — what it means
- Cancer risk — the real picture
- How children's immune systems clear HPV
- Treatment options
- The HPV vaccine — the most important protection
- When to see a doctor
- Frequently asked questions
Types of HPV Most Common in Children
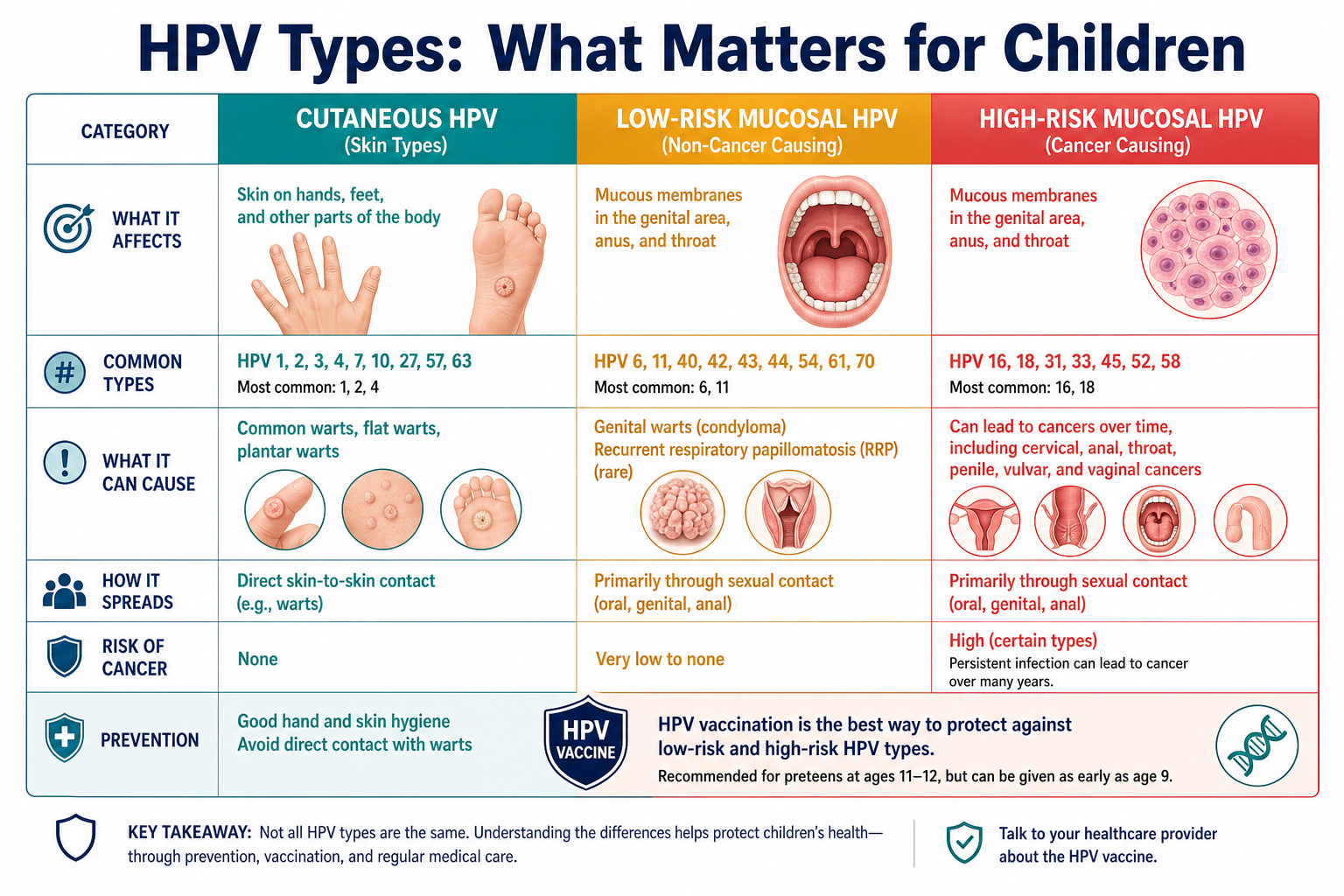
There are more than 200 known types of human papillomavirus, and the type a child is most likely to encounter is nothing like the strains adults worry about. The critical distinction for parents is between cutaneous HPV — which infects the outer skin — and mucosal HPV, which infects the soft tissue linings of the genitals, throat, and mouth.
According to the CDC HPV fact sheet{:target="_blank"}, HPV is the most common viral infection of the skin and mucous membranes in humans. In children, the vast majority of infections are cutaneous — producing common warts, plantar warts, and flat warts. These are HPV infections in the technical sense, but they carry no meaningful health risk and are not sexually transmitted.
| HPV Category | Examples | Common in Children? | Health Risk |
|---|---|---|---|
| Cutaneous (skin) | Common warts, plantar warts, flat warts | Very common | None — harmless, usually self-resolving |
| Low-risk mucosal | Types 6, 11 | Uncommon | Genital warts, recurrent respiratory papillomatosis — not cancer |
| High-risk mucosal | Types 16, 18 | Rare in children | Cancer only after persistent infection over many years |
The public conflation of "wart" with "STI" is one of the most persistent sources of unnecessary parental distress. When a child develops a wart on their hand or foot, they have an HPV infection — but it is no more medically significant than a cold sore, and it requires no different social response.
How Children Get HPV
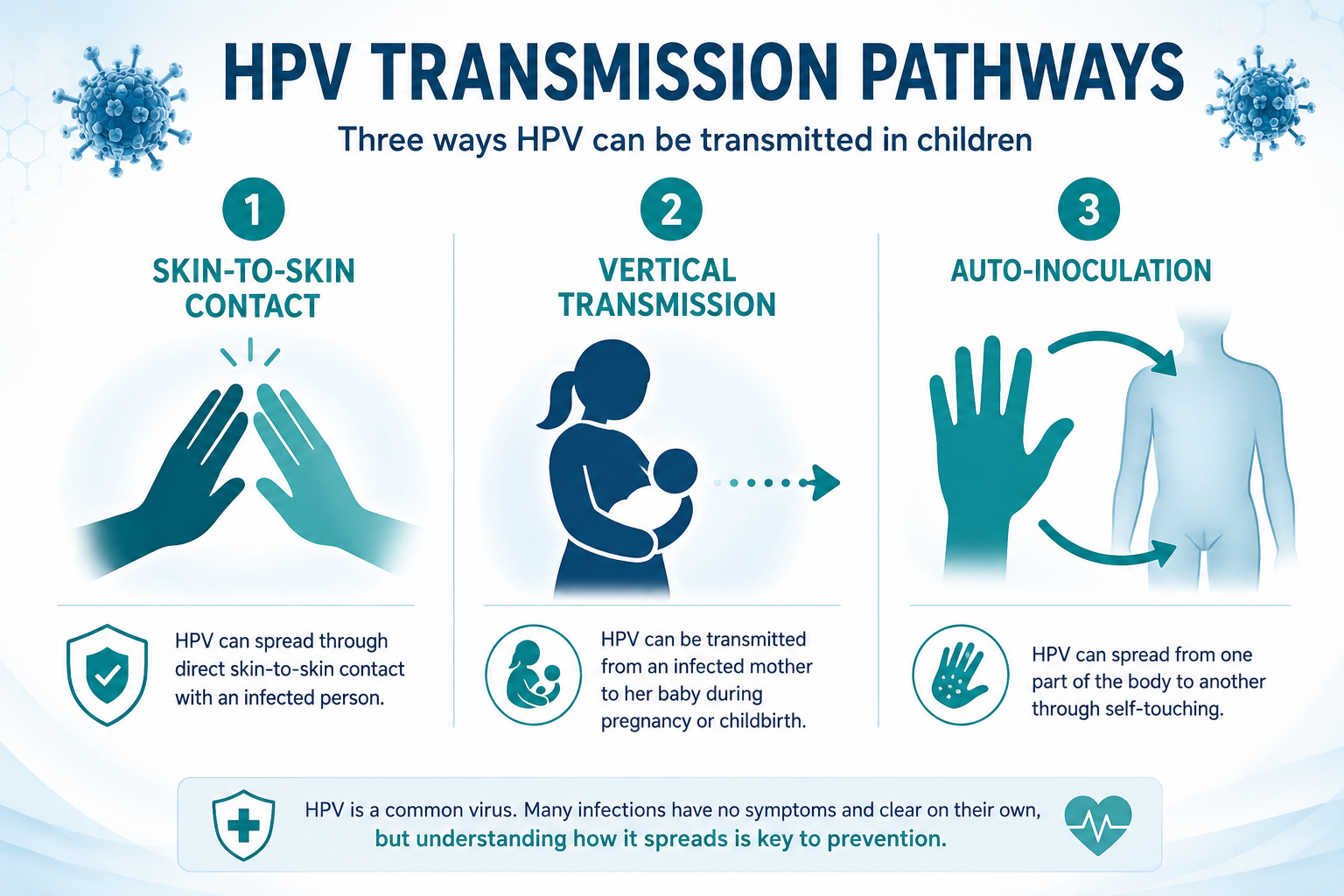
For cutaneous HPV, the route is simple: direct skin-to-skin contact with an infected surface. Children touch shared objects, play in close physical contact, and frequently have minor cuts or abrasions through which the virus can enter. HPV can survive on surfaces for several hours to days, which means shared towels, gym floors, and swimming pool surrounds can all serve as transmission points for cutaneous strains. This is ordinary childhood behavior, not a sign of anything abnormal.
Vertical transmission is a separate and documented route for mucosal HPV. A mother with an active HPV infection can transmit the virus to her infant during vaginal delivery. In most cases, this produces no symptoms in the infant. In rare cases, it can cause recurrent respiratory papillomatosis (RRP) — benign but recurrent growths in the larynx and throat caused by HPV types 6 and 11. RRP is uncommon, but when it occurs it requires specialist management and can be serious. The WHO HPV fact sheet{:target="_blank"} notes that vertical transmission, while real, is not a reason to recommend caesarean delivery solely to prevent HPV transmission.
Auto-inoculation is another route that explains patterns parents sometimes find confusing. A child with a wart on one hand can transfer the virus to another area of their own body — their face, their other hand, or elsewhere — simply by touching the wart and then touching another skin surface. This is how warts spread from one finger to several fingers, or from hands to the face. It involves no external exposure.
For a comprehensive look at how HPV spreads beyond these childhood-specific routes, can you get HPV without having sex covers the full transmission picture in detail.
Symptoms in Children and Adolescents
For the majority of children with HPV, there are no symptoms at all — the immune system clears the infection before it produces any visible sign. When symptoms do appear, they depend entirely on which type of HPV is involved and where on the body it has taken hold.
Cutaneous HPV produces the warts most parents are familiar with:
- Common warts — rough-surfaced, firm, skin-colored bumps most often found on the hands, fingers, and around the nails. They may have a cauliflower-like texture.
- Plantar warts — warts that grow on the soles of the feet, sometimes growing inward due to the pressure of walking. They can cause discomfort or pain with activity.
- Flat warts — smaller, smoother, and flatter than common warts, often appearing in clusters on the face, legs, or backs of hands. They are more common in children and adolescents than in adults.
Mucosal HPV produces different presentations. Oral warts caused by low-risk HPV types may appear as soft, painless bumps inside the mouth or on the lips. These are uncommon in children and should be evaluated by a clinician. For more on HPV affecting the mouth and throat, oral HPV: the silent infection no one talks about provides detailed context.
High-risk HPV types — the strains associated with cancer — produce no visible symptoms whatsoever. They cannot be identified through visual examination. In practice, high-risk HPV is rarely clinically relevant in children under 12, and its detection in a young child always warrants specialist evaluation.
Genital HPV in Children — What It Means
This section requires particular care, because the clinical reality is more nuanced than either extreme — neither "this is definitely abuse" nor "this is definitely harmless" — and parents deserve an accurate picture.
Genital HPV in a prepubescent child can occur through non-sexual routes. Vertical transmission from mother to infant during birth is a documented mechanism, and auto-inoculation — a child transferring HPV from a wart on their hand to the genital area while bathing or toileting — is possible. These are real, medically recognized pathways.
However, the presence of genital HPV in a prepubescent child requires evaluation by a trained healthcare provider, and in many cases referral to a specialist in child abuse assessment. This is not because sexual abuse is the assumed cause — it is because the possibility must be properly and professionally evaluated to protect the child. The presence of genital HPV alone does not confirm sexual abuse. The absence of other clinical indicators of abuse means that non-sexual transmission may be the most likely explanation in a given case. But that determination must be made by clinicians trained to conduct these evaluations sensitively and accurately — not assumed by a parent at home.
If a child has any genital lesions or warts, the appropriate response is prompt medical evaluation — not reassurance, and not home treatment.
The evaluation process, when conducted by experienced professionals, is designed to be as gentle and non-traumatic as possible for the child. A pediatrician is the right first contact, and they will refer to appropriate specialists — which may include pediatric gynecology, pediatric urology, or a child abuse assessment team — based on what they find.
For adolescents who have become sexually active, genital HPV is managed through the same clinical pathways as adult HPV: medical evaluation, appropriate monitoring, and treatment of visible warts where needed.
Cancer Risk — The Real Picture
HPV-related cancer in children is extremely rare, and understanding why requires understanding the biology. HPV causes cancer only when a high-risk strain — most commonly types 16 and 18 — establishes a persistent infection that the immune system fails to clear over an extended period, typically a decade or more. The virus must then cause cellular changes that progress through several precancerous stages before invasive cancer develops.
Children who acquire HPV almost always clear it naturally. The timeline to cancer development is so long that even adolescents who acquire a high-risk strain during their teenage years have ample time for clearance before any cancer risk becomes clinically meaningful — provided they receive appropriate monitoring as they enter adulthood.
For context on how this process unfolds at the cellular level, how does HPV cause cancer explains the mechanism in detail. For a specific look at the highest-risk strains, why HPV 16 and HPV 18 are the most dangerous HPV strains covers what makes these types particularly concerning in adult populations.
The National Cancer Institute{:target="_blank"} notes that while HPV is responsible for nearly all cervical cancers and a significant proportion of other anogenital and oropharyngeal cancers, these outcomes occur predominantly in adults with persistent, uncleared infections — not in children.
Cervical cancer screening does not begin until age 21 per standard clinical guidelines from the CDC and ACOG. Adolescents with specific risk factors or known persistent high-risk infection may warrant earlier evaluation, which a clinician can advise on individually.
The appropriate response to this low cancer risk in children is not complacency — it is vaccination. The vaccine prevents the infections that, if left unchecked over decades, could eventually become cancer. The rarity of pediatric HPV-related cancer is not a reason to delay vaccination; it is evidence that the immune system can clear HPV when supported — and vaccination gives that immune system a decisive head start.
How Children's Immune Systems Clear HPV
Children and adolescents generally clear HPV faster than adults, and this is not simply reassuring language — it reflects documented immunological differences. Young immune systems are more actively responsive to new antigens, mounting stronger and faster adaptive immune responses when encountering a pathogen for the first time.
Most common warts in children resolve spontaneously within one to two years without any treatment. Studies of mucosal HPV in adolescents similarly show clearance rates that are considerably higher than those observed in adults over 30, with most infections clearing within one to two years in immunocompetent young people.
The lifestyle factors that support immune function in children are the same ones that matter across all age groups:
- Adequate sleep — immune function is directly linked to sleep quality and duration; school-age children need 9–12 hours per night, adolescents 8–10 hours
- Nutrient-rich diet — particularly adequate vitamin D, zinc, and folate, which are directly involved in immune cell function
- Regular physical activity — moderate exercise supports immune surveillance
- Reduced psychological stress — chronic stress suppresses immune function in children and adolescents just as it does in adults
These are appropriate general health recommendations for any child, regardless of HPV status. No specific supplement is recommended for children or adolescents with HPV — no such recommendation is clinically supported by published evidence.
Treatment Options
Treatment decisions for HPV in children depend entirely on the type of infection, its location, and whether it is causing symptoms or complications.
Watchful waiting is the appropriate first approach for most uncomplicated cutaneous warts. The majority of common warts in children disappear within one to two years without any intervention. Treatment is not medically necessary for a harmless wart on a child's hand — it is an option when the wart is causing distress, pain, or practical difficulty.
Wart removal becomes relevant for persistent, painful, spreading, or cosmetically distressing warts. Options include:
- Salicylic acid — an over-the-counter topical treatment applied daily to the wart. It works by gradually breaking down the wart tissue. It is safe for children when used as directed but requires consistent application over weeks to months.
- Cryotherapy — freezing of the wart with liquid nitrogen, performed by a clinician. Often requires multiple sessions. Can be uncomfortable for young children.
- Laser removal or minor surgical procedures — reserved for warts that have not responded to other treatments. Performed by a dermatologist.
An important point for parents: treatment removes the visible wart — it does not eliminate HPV from the body. Recurrence is possible after any treatment. This does not mean treatment has failed; it means the immune system has not yet fully cleared the underlying virus.
Specialist management is required for oral or genital HPV presentations in children. Parents should not attempt to treat these at home. A pediatrician will refer to appropriate specialists — dermatology, pediatric gynecology, pediatric urology, or ENT — depending on the presentation.
Recurrent respiratory papillomatosis (RRP), caused by HPV types 6 and 11 acquired through vertical transmission, is a rare but serious condition. It produces benign growths in the larynx and throat that can obstruct the airway and affect the voice. Management requires specialist ENT care and typically involves surgical removal of growths, often repeated procedures over time. RRP is not cancer, but it is a condition that requires ongoing specialist involvement and should not be minimized.
The HPV Vaccine — The Most Important Protection
The HPV vaccine (Gardasil 9) is among the most effective cancer prevention tools in modern medicine, and it is strongly recommended for preteens by the CDC, the American Academy of Pediatrics (AAP), the World Health Organization, and the American College of Obstetricians and Gynecologists (ACOG).
Recommended timing: Ages 11–12, with the option to start as early as age 9. The reason for vaccinating before the teenage years is straightforward — the vaccine works best before any exposure to HPV has occurred, and immune response to the vaccine is strongest in younger adolescents.
Dosing schedule:
- Ages 9–14: 2 doses, given 6–12 months apart
- Ages 15 and older: 3 doses, given over 6 months
What Gardasil 9 protects against: HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. This covers the two strains responsible for approximately 70% of cervical cancers (types 16 and 18), the two strains responsible for most genital warts (types 6 and 11), and five additional high-risk strains linked to other cancers.
The vaccine does not treat existing HPV infection. It is a prevention tool, not a treatment. This is why timing matters — vaccination after exposure to a covered strain will not clear that strain.
The vaccine benefits both boys and girls. Boys vaccinated against HPV are protected against HPV-related anal cancer, penile cancer, and oropharyngeal (throat) cancer. They also cannot transmit covered strains to sexual partners — meaning vaccinated boys contribute directly to population-level protection.
The CDC HPV vaccine information for parents{:target="_blank"} and the AAP HPV vaccine recommendations{:target="_blank"} provide detailed guidance on the schedule, safety data, and how to discuss the vaccine with children and adolescents. The safety profile of Gardasil 9 has been extensively studied across millions of doses administered worldwide. The vaccine is safe, effective, and one of the most important preventive health decisions a parent can make for their child.
When to See a Doctor
Not every wart requires a doctor's visit, but several situations involving HPV in children warrant prompt medical evaluation. Parents should seek professional assessment in any of the following circumstances:
- Any genital lesions or bumps in a child — do not wait, do not attempt home treatment, and do not assume the cause. Prompt evaluation by a pediatrician is the appropriate first step.
- Warts in the mouth or throat — these require ENT referral and should not be managed at home.
- Warts that are rapidly spreading, painful, bleeding, or interfering with daily activities — including plantar warts that make walking difficult.
- Warts that return repeatedly after treatment — recurrence may indicate that the immune system needs additional support or that a different treatment approach is warranted.
- Any concern that a child may have experienced sexual abuse — if genital HPV is discovered alongside other indicators of concern, or if a child has disclosed anything that raises concern, a trained child abuse assessment team should be involved. The pediatrician is the right first contact.
- Adolescents who become sexually active — HPV vaccination should be completed if it has not been, and age-appropriate STI screening should be discussed with a clinician.
- Symptoms of RRP — a child with a persistently hoarse voice, noisy breathing, or difficulty breathing that cannot be explained by illness should be evaluated by an ENT specialist.
Frequently Asked Questions
Can a child get HPV from a swimming pool or a shared towel?
HPV can survive on surfaces for several hours to days, which means transmission through shared towels, pool surrounds, and changing room floors is plausible for cutaneous strains. This is one of the reasons common warts are so prevalent among school-age children — ordinary shared environments are sufficient for transmission. The risk can be reduced by not sharing towels and wearing footwear in communal changing areas, but these are practical precautions rather than causes for alarm. Cutaneous HPV acquired this way is medically harmless.
If my child has warts, do they have an STI?
No. Common warts, plantar warts, and flat warts are caused by cutaneous HPV types that are not sexually transmitted. They are spread through ordinary skin contact and are one of the most common infections of childhood. The presence of warts on a child's hands or feet has no connection to sexual activity and carries no social stigma. The association between HPV and sexually transmitted infection applies specifically to mucosal HPV types — not to the cutaneous types responsible for ordinary warts.
Can HPV be transmitted from a mother to her baby?
Yes, vertical transmission is documented. A mother with an active HPV infection can transmit the virus to her infant during vaginal delivery. In most cases, the infant's immune system clears the infection without any symptoms. In rare cases, the infant may develop recurrent respiratory papillomatosis (RRP) — growths in the throat caused by HPV types 6 and 11. RRP requires specialist management but is not cancer. The risk of vertical transmission is not considered sufficient justification for caesarean delivery solely to prevent HPV, according to current guidelines from the WHO and ACOG.
At what age should my child get the HPV vaccine?
The CDC and AAP recommend the HPV vaccine at ages 11–12, with the option to start as early as age 9. Two doses are given for children who start the series before age 15; three doses are required for those who start at age 15 or older. Vaccination before first exposure to HPV produces the strongest immune response and provides the most complete protection. If your child has not been vaccinated, speak with their pediatrician — the vaccine can still be given up to age 26 for those who missed it during the recommended window, and in some cases up to age 45 after a clinical discussion.
My adolescent daughter was diagnosed with HPV — what do I do?
The first step is to remain calm and schedule an appointment with her gynecologist or a clinician experienced in adolescent health. Most HPV infections in adolescents clear naturally within one to two years without any treatment. The clinician will assess which HPV type is involved, whether any visible lesions are present, and what monitoring is appropriate. Cervical cancer screening does not typically begin until age 21, but a clinician may recommend earlier evaluation depending on the specific circumstances. Ensure that her HPV vaccination series is complete if it is not already. Support her with honest, non-alarmist information — an HPV diagnosis in an adolescent is common and, in most cases, resolves without lasting consequences.
Conclusion
HPV in children is far more common — and far less alarming — than most parents initially fear. The vast majority of pediatric HPV infections are cutaneous warts that resolve on their own, cause no health consequences, and require nothing more than watchful waiting. Understanding this distinction is the foundation of a calm, informed response.
At the same time, certain presentations of HPV in children do require prompt and professional attention — and this article has tried to be clear about where those lines fall. Genital HPV in a prepubescent child always warrants medical evaluation. Oral or throat warts require specialist referral. Recurrent respiratory papillomatosis requires ongoing ENT management. And any concern about a child's safety or wellbeing should be routed immediately to trained professionals.
Practical next steps for parents:
- Check vaccination status. If your child is between 9 and 12 years old and has not started the HPV vaccine series, speak with their pediatrician at the next visit. This is the single most impactful preventive action available.
- Distinguish wart type before worrying. A rough bump on a child's hand or foot is almost certainly a cutaneous wart — medically harmless and extremely common. Consult a clinician if you are unsure.
- Do not attempt to diagnose or treat genital lesions at home. Any genital lesion in a child requires prompt medical evaluation, full stop.
- Support general immune health through lifestyle. Adequate sleep, a nutrient-rich diet, regular physical activity, and reduced stress all support the immune function that clears HPV naturally — in children as in adults.
- Keep follow-up appointments. For adolescents with a known HPV diagnosis, regular monitoring with a clinician is the appropriate long-term approach. Do not skip follow-up visits.
Related Reading
For parents and adults who want to understand HPV more broadly, the following articles provide evidence-based information on related topics:
- Can you get HPV without having sex? — a detailed look at non-sexual HPV transmission routes
- How does HPV cause cancer? — the cellular mechanism explained clearly
- Oral HPV: the silent infection no one talks about — HPV in the mouth and throat, symptoms, and what to do
- Why HPV 16 and HPV 18 are the most dangerous HPV strains — what makes high-risk strains clinically significant
References
- Centers for Disease Control and Prevention. HPV vaccine information for parents. https://www.cdc.gov/hpv/parents/index.html
- Centers for Disease Control and Prevention. Human papillomavirus (HPV). https://www.cdc.gov/hpv
- American Academy of Pediatrics. HPV vaccine recommendations. https://www.aap.org/en/patient-care/immunizations/hpv/
- World Health Organization. Human papillomavirus (HPV) and cervical cancer. https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer
- National Cancer Institute. HPV and cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







