


A positive HPV result is one of the most anxiety-producing pieces of medical news a person can receive — and the first thing most people do is search "how does HPV cause cancer." That instinct is actually a healthy one, because understanding the biology makes one fact immediately clear: the path from HPV infection to cancer is slow, rare, and interceptable at multiple points. Most people who carry HPV will never develop cancer from it. What follows is a plain-language explanation of the mechanism — not to minimize a real concern, but to replace fear with accurate information.
Key Takeaways
- Approximately 90% of HPV infections clear on their own within two years without causing any harm.
- Cancer requires a very specific sequence: a high-risk HPV strain, persistent infection over many years, and cellular changes that go undetected and untreated.
- HPV causes cancer by producing two proteins — E6 and E7 — that disable the cell's natural tumor-suppression systems.
- CIN (cervical intraepithelial neoplasia) is a precancerous cellular change, not cancer. It is detectable, treatable, and often regresses on its own.
- The entire process from initial infection to invasive cancer typically takes 10 to 20 years — which is precisely why regular screening is so effective at preventing it.
In This Article
- Most HPV never causes cancer
- Step 1 — How HPV infects cells
- Step 2 — How HPV hijacks cell controls
- Step 3 — Precancerous changes (CIN)
- Step 4 — When cancer develops
- Which cancers are linked to HPV?
- How long does the process take?
- Why do some infections progress and others don't?
- Prevention — how to interrupt the process
- Frequently asked questions
Most HPV Never Causes Cancer
Before explaining how HPV causes cancer, it is worth stating plainly what the data actually show: the overwhelming majority of HPV infections never cause cancer at all. According to the CDC, approximately 90% of HPV infections clear within two years without treatment and without causing any lasting harm. The immune system identifies the virus and eliminates it — quietly, without symptoms, and often without the person ever knowing they were infected.
Cancer is not the default outcome of HPV. It is the outcome of a rare, specific, and slow sequence of events that requires all of the following to occur simultaneously:
- Infection with a high-risk HPV strain (not all strains carry cancer risk)
- Persistent infection that the immune system fails to clear over years
- Progressive cellular damage that goes undetected and untreated
Most HPV infections never satisfy all three conditions. Understanding why requires a closer look at the biology.
Step 1 — How HPV Infects Cells
HPV is a small, non-enveloped DNA virus. It enters the body through microscopic breaks in skin or mucous membranes — the kind that occur during normal sexual contact. Once inside, it targets a specific type of cell: basal epithelial cells, which sit at the deepest layer of surface tissue and divide continuously to replenish the cells above them.
The virus attaches to receptors on the surface of these basal cells, enters the cell, and travels to the nucleus. There, it inserts its own genetic material and uses the cell's existing machinery to replicate itself. In most cases, the immune system recognizes viral proteins on the surface of infected cells and mounts a response that clears the infection within months.
In a smaller subset of cases, the virus is not cleared. It remains integrated into the host cell's DNA, replicating silently with each cell division. This is what clinicians mean by persistent infection — and it is the necessary first condition for cancer risk to exist. Without persistence, the process stops here.
Step 2 — How HPV Hijacks Cell Controls
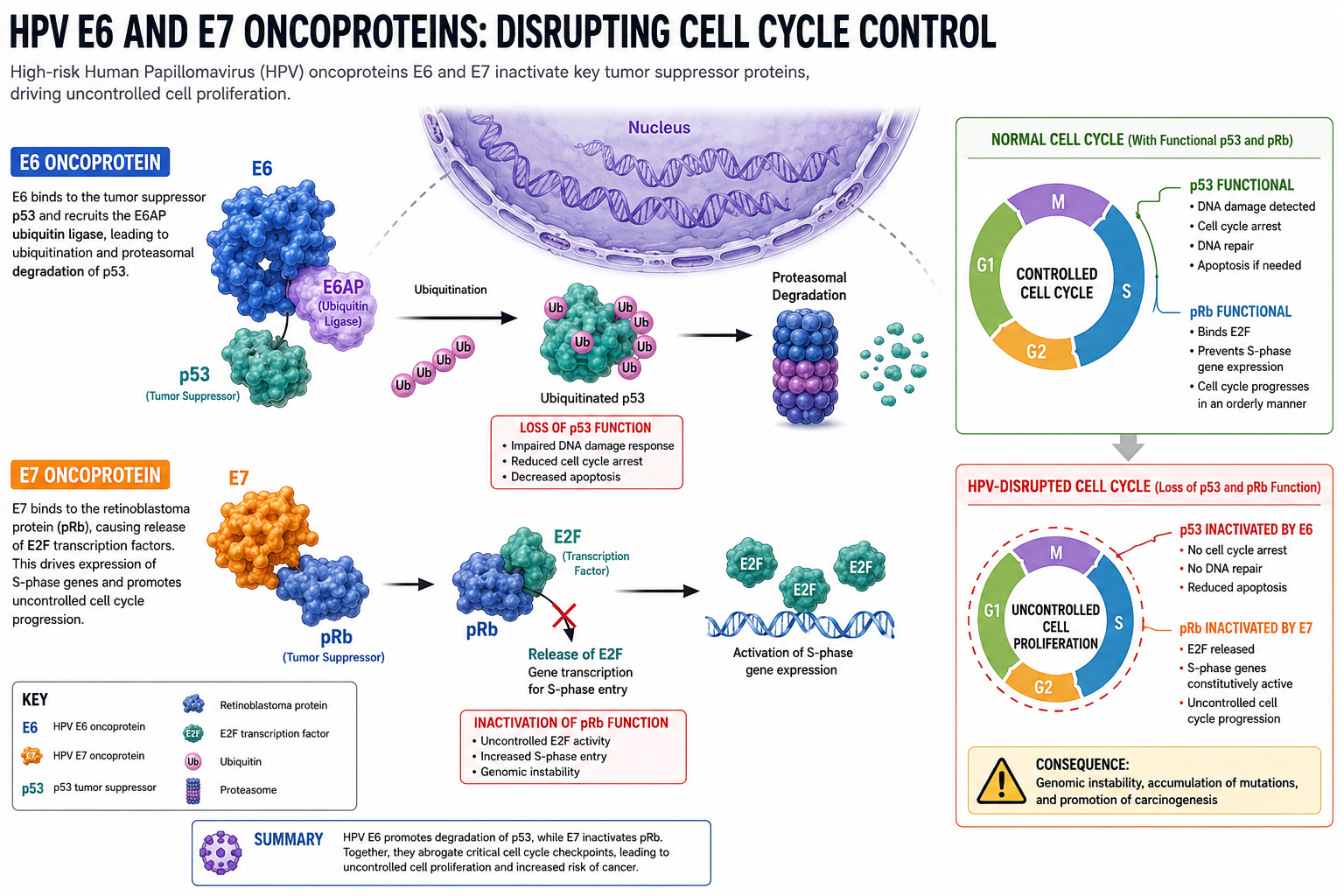
This section contains the most important biology for understanding how HPV causes cancer. When high-risk HPV strains persist inside cells, they begin producing two proteins that directly interfere with the cell's ability to regulate its own growth: E6 and E7.
What E6 does
Every healthy cell contains a protein called p53, often described as the "guardian of the genome." When a cell's DNA is damaged — by radiation, toxins, replication errors, or viral interference — p53 detects that damage and does one of two things: it halts cell division to allow repair, or it triggers apoptosis (programmed cell death) if the damage is too severe to fix. p53 is, in effect, the cell's self-destruct mechanism when things go wrong.
HPV's E6 protein binds directly to p53 and marks it for degradation. The cell's own disposal machinery then breaks it down. With p53 gone, DNA-damaged cells no longer receive the signal to stop dividing or self-destruct. They survive when they should not.
What E7 does
The second tumor-suppressor system is controlled by a protein called pRb (retinoblastoma protein). Under normal conditions, pRb acts as a brake on cell division. It holds a transcription factor called E2F in an inactive state, preventing the cell from entering the division cycle until conditions are appropriate. When growth signals arrive and conditions are right, pRb releases E2F and division proceeds in a controlled way.
HPV's E7 protein binds to pRb and inactivates it. The brake is released permanently. Cells begin dividing without the normal checks that govern when and how often division should occur.
The combined effect
Think of it this way: p53 is the airbag system — it deploys when something goes wrong to prevent catastrophic damage. pRb is the brake — it controls speed and prevents runaway acceleration. E6 disables the airbags. E7 cuts the brakes. With both systems compromised, cells that carry genetic errors survive, divide, pass those errors to daughter cells, and accumulate further mutations with each generation.
This accumulation of mutations over time is what drives the progression toward cancer. It does not happen overnight. It takes years — sometimes decades.
Key point: Low-risk HPV strains (such as HPV-6 and HPV-11, which cause genital warts) produce versions of E6 and E7 that bind much less effectively to p53 and pRb. This is the primary reason they do not cause cancer. High-risk strains — particularly HPV-16 and HPV-18 — produce E6 and E7 variants with far greater binding affinity, which is what makes them oncogenic.
Step 3 — Precancerous Changes (CIN)
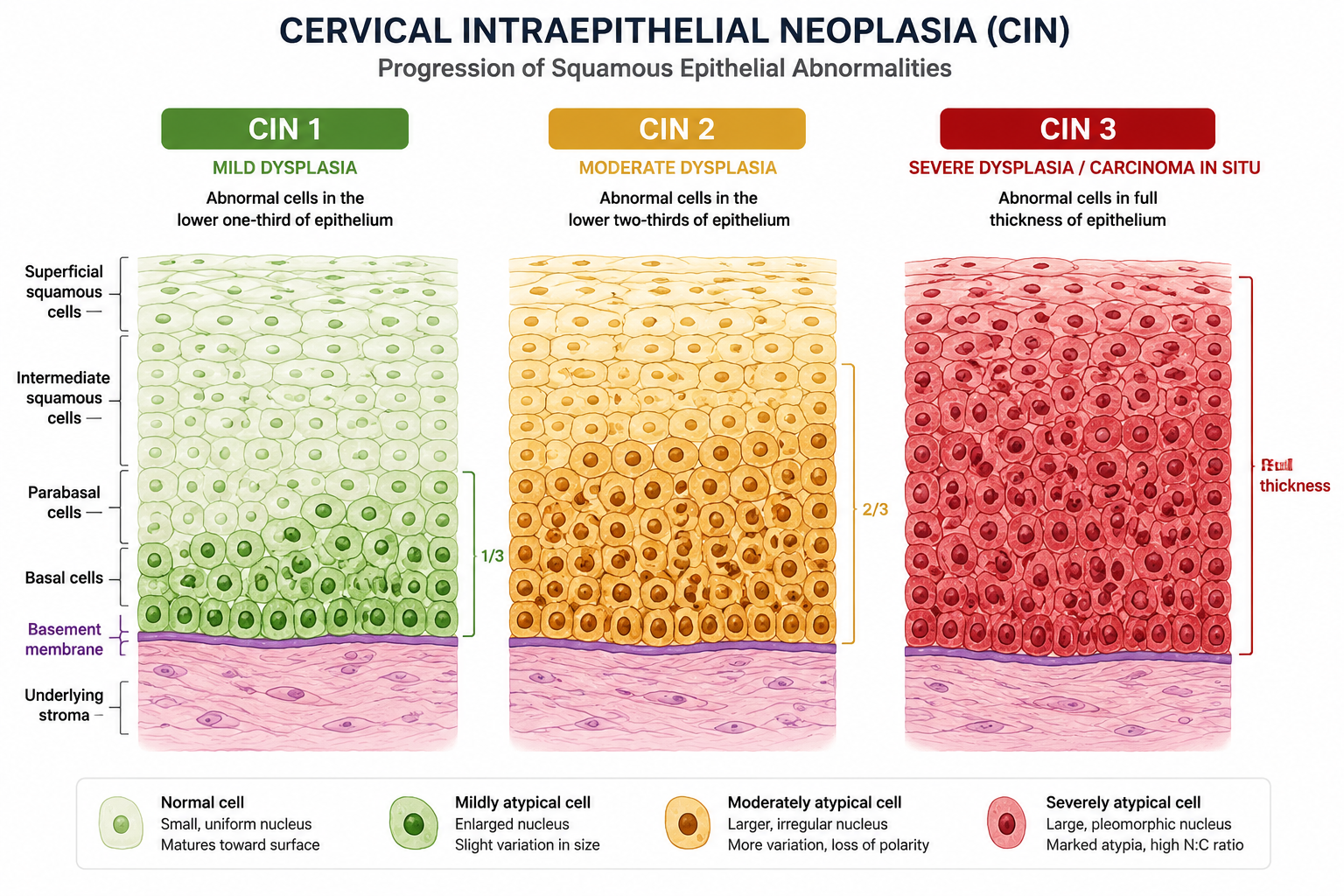
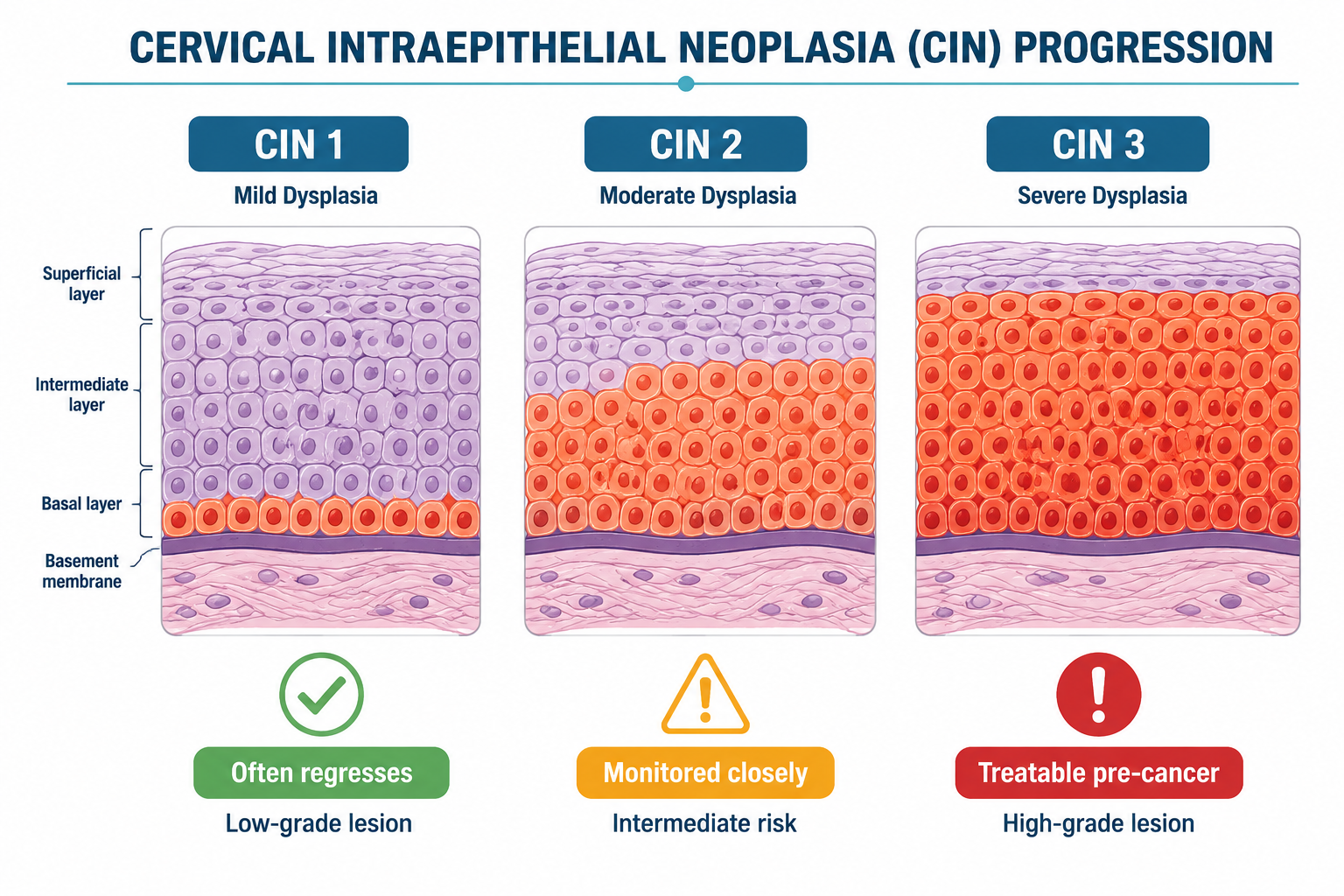
As abnormal cells accumulate in cervical tissue, pathologists can observe and classify the degree of cellular disorganization. This classification system is called CIN — cervical intraepithelial neoplasia. It is critical to understand that CIN is not cancer. It is a description of cellular abnormality that exists on a spectrum.
| CIN Stage | Description | Typical Outcome |
|---|---|---|
| CIN 1 | Mild cellular changes; abnormal cells in the lower third of the epithelium | ~60–70% regress spontaneously within 2 years |
| CIN 2 | Moderate changes; abnormal cells in the lower two-thirds | ~40–50% regress; monitored closely or treated |
| CIN 3 | Severe changes; abnormal cells throughout the full epithelial thickness | Lower spontaneous regression rate; treatment typically recommended |
CIN 1 is the most common finding after an abnormal Pap result, and the majority of CIN 1 cases resolve without any intervention as the immune system clears the underlying HPV infection. CIN 2 and CIN 3 represent progressively more significant cellular disruption, but they remain pre-invasive — meaning the abnormal cells have not yet broken through the basement membrane that separates surface epithelium from deeper tissue.
This distinction matters enormously. The entire purpose of cervical screening — the Pap smear and HPV co-test — is to detect cellular changes at the CIN stage, when they are still treatable and have not yet become invasive cancer. According to NCI cervical cancer screening guidelines, regular screening dramatically reduces cervical cancer incidence and mortality precisely because this pre-invasive window is wide and detectable.
If you have received a CIN diagnosis, you have not been diagnosed with cancer. You have been given advance warning of a cellular process that can be monitored and, if necessary, treated effectively.
Step 4 — When Cancer Develops
Invasive cancer develops when abnormal cells breach the basement membrane — the thin structural layer that separates surface epithelium from the connective tissue and blood vessels beneath it. Once cells cross that boundary, they gain access to the lymphatic and circulatory systems, which creates the possibility of spread to other parts of the body.
By the time invasive cancer develops, the cells involved have typically undergone several additional changes beyond E6/E7 disruption:
- Telomerase activation — normally, cells can only divide a finite number of times before their chromosomal end-caps (telomeres) shorten to the point of triggering senescence. Cancer cells reactivate telomerase, an enzyme that rebuilds telomeres, effectively making them immortal.
- Angiogenesis — growing tumors require a blood supply. Cancer cells secrete signaling molecules that stimulate the growth of new blood vessels into the tumor mass.
- Immune evasion — advanced cancer cells develop mechanisms to avoid detection and destruction by immune cells, including downregulating the surface proteins that normally flag them for elimination.
This is a multi-step process that requires years of unchecked cellular progression. Reaching this stage is not inevitable — it requires that every prior opportunity for detection and intervention has been missed. That is why the emphasis on regular screening is not merely precautionary language. It reflects the genuine biology of how HPV causes cancer and where the process can be stopped.
Which Cancers Are Linked to HPV?
According to the World Health Organization, HPV is responsible for approximately 5% of all cancers worldwide. Cervical cancer is the most extensively studied, but HPV is causally linked to cancers at several anatomical sites in both women and men.
| Cancer Type | HPV Attribution | Primary Strains |
|---|---|---|
| Cervical | ~99% | 16, 18, 31, 45 |
| Oropharyngeal (throat) | ~70% | 16 |
| Anal | ~90% | 16, 18 |
| Vulvar | ~25% | 16, 18 |
| Vaginal | ~65% | 16, 18 |
| Penile | ~50% | 16, 18 |
Sources: NCI — HPV and Cancer
HPV-16 and HPV-18 together account for the majority of HPV-attributable cancers across all sites. For a detailed breakdown of why these two strains carry disproportionate risk, see why HPV 16 and HPV 18 are the most dangerous HPV strains.
Oropharyngeal cancer — cancer of the back of the throat, base of the tongue, and tonsils — deserves particular attention because its incidence has been rising and it often presents without early symptoms. For a thorough explanation of how HPV affects the oral cavity and throat, oral HPV: the silent infection no one talks about covers the transmission, detection, and risk factors in full.
How Long Does the Process Take?
The progression from initial HPV infection to invasive cancer is measured in decades, not months or years. The general timeline looks like this:
- Initial infection — HPV enters basal epithelial cells. Most infections are cleared by the immune system within 6–24 months.
- Persistent infection (approximately 2–5 years) — In a minority of cases, the immune system does not clear the virus. The infection becomes established in host cell DNA.
- Precancerous cellular changes (approximately 5–10 years after persistent infection) — E6 and E7 proteins begin disrupting p53 and pRb. CIN changes become detectable on screening.
- Invasive cancer (approximately 10–20 years after initial infection) — Cellular changes progress through CIN 3 and breach the basement membrane, at which point invasive cancer is present.
The 10-to-20-year window between infection and invasive cancer is not a source of complacency — it is the reason that screening programs are so effective. A Pap smear or HPV co-test conducted every three to five years, as recommended, creates multiple opportunities to detect CIN changes and intervene long before cancer develops.
Why Do Some Infections Progress and Others Don't?
Given that most HPV infections clear without incident, the relevant question is: what distinguishes the minority of cases that progress? Several factors influence whether an infection becomes persistent and whether persistent infection advances toward precancerous change.
HPV strain is the most significant determinant. High-risk strains — particularly HPV-16 — produce E6 and E7 proteins with substantially greater oncogenic activity than low-risk strains. The strain a person carries is the single largest predictor of cancer risk.
Immune competence is the second major factor. A robust immune system is the primary mechanism by which HPV is cleared. People who are immunocompromised — due to HIV infection, organ transplantation, long-term corticosteroid use, or other causes — have significantly higher rates of persistent HPV and HPV-related cancer.
Smoking is the strongest modifiable lifestyle co-factor. Tobacco carcinogens accumulate in cervical mucus and directly damage cervical epithelial cells, compounding the DNA damage caused by E6/E7. Smokers with high-risk HPV have substantially higher rates of CIN progression than non-smokers.
Nutritional status also appears to matter. Deficiencies in folate and vitamin D have been associated with higher rates of HPV persistence and CIN progression in observational studies, though the causal relationships are not fully established.
Duration of infection compounds all of the above. The longer a high-risk HPV infection persists, the greater the cumulative cellular damage and the higher the probability of progression.
For a detailed exploration of why some immune systems fail to clear HPV when others succeed, why HPV doesn't clear in some people covers the immunological and lifestyle factors in depth.
Prevention — How to Interrupt the Process
Understanding how HPV causes cancer also reveals exactly where the process can be interrupted. There are three evidence-based strategies.
1. Vaccination
The Gardasil 9 vaccine provides protection against nine HPV strains, including HPV-16, HPV-18, and five additional high-risk types that together account for approximately 90% of HPV-attributable cervical cancers. Vaccination prevents new infection — it does not treat an existing one. It is most effective when administered before first sexual exposure, but current guidelines extend the recommended age range to 26 for all adults, and vaccination may be considered up to age 45 in consultation with a healthcare provider.
2. Regular screening
Routine Pap smears and HPV co-testing are the most powerful tools available for preventing cervical cancer in people who are already sexually active. Because the progression from infection to invasive cancer takes 10 to 20 years, regular screening creates a wide detection window. CIN changes identified through screening are highly treatable, with excellent outcomes.
3. Immune support and lifestyle
Smoking cessation is the most impactful lifestyle change a person with high-risk HPV can make. The evidence linking smoking to accelerated CIN progression is consistent and substantial.
Beyond smoking cessation, supporting immune function through sleep, nutrition, stress management, and targeted supplementation is an area of active research. One supplement — AHCC (Active Hexose Correlated Compound) — has been studied specifically in the context of HPV clearance. A published human clinical trial conducted by Dr. Judith Smith at the University of Texas Health Science Center at Houston found that AHCC supplementation was associated with HPV clearance in a subset of participants. This research is promising and preliminary — AHCC is not FDA-approved as an HPV treatment, and it should not be characterized as a proven cancer prevention strategy. However, it represents the most rigorous human clinical evidence currently available for any supplement in this context.
NovaHerbs AHCC (700 mg per capsule) is manufactured in a GMP-certified facility in the USA. The clinical research protocol used 3 grams per day taken on an empty stomach for a minimum of six months — approximately four to five capsules daily at that dose. For a thorough review of the evidence behind AHCC and HPV, does AHCC really help clear HPV? What the research actually says covers the clinical data in full.
For a broader overview of natural strategies to support HPV clearance, how to clear HPV naturally outlines ten evidence-informed approaches.
Frequently Asked Questions
Does everyone with HPV get cancer?
No. The vast majority of people with HPV do not develop cancer. According to the CDC, approximately 90% of HPV infections clear within two years without causing harm. Cancer requires a specific, rare combination of factors: a high-risk strain, persistent infection, and years of undetected cellular progression. Most HPV infections never satisfy all three conditions. Regular screening further reduces the likelihood that any precancerous changes go undetected.
How long does it take for HPV to cause cancer?
The process typically takes 10 to 20 years from initial infection to invasive cancer. This long timeline includes a period of persistent infection, followed by gradual precancerous cellular changes (CIN), and finally the breach of the basement membrane that defines invasive cancer. The extended timeline is the reason that regular cervical screening is so effective — there are multiple years during which abnormal changes can be detected and treated before they become cancer.
What is the difference between CIN and cancer?
CIN (cervical intraepithelial neoplasia) describes abnormal cellular changes confined to the surface layer of cervical tissue. It is a pre-invasive condition — the abnormal cells have not broken through the basement membrane into deeper tissue. CIN is not cancer. It is a detectable, treatable cellular change that may regress on its own, remain stable, or — if untreated over many years — progress toward cancer. A CIN diagnosis is a reason for monitoring and possible treatment, not a cancer diagnosis.
Which HPV strains cause cancer?
Not all HPV strains carry cancer risk. Of the more than 200 known HPV types, approximately 14 are classified as high-risk oncogenic strains. HPV-16 and HPV-18 are responsible for the majority of HPV-attributable cancers — together accounting for roughly 70% of cervical cancers. Other high-risk strains include HPV-31, HPV-33, HPV-45, HPV-52, and HPV-58. Low-risk strains such as HPV-6 and HPV-11 cause genital warts but do not cause cancer.
Can HPV-related cancer be prevented?
Yes, through multiple overlapping strategies. Vaccination with Gardasil 9 prevents infection with the most dangerous HPV strains. Regular cervical screening detects precancerous CIN changes before they become invasive. Smoking cessation reduces the rate of CIN progression. Maintaining strong immune function — through sleep, nutrition, and where appropriate, targeted supplementation — supports the body's natural ability to clear persistent infections. None of these strategies is a guarantee, but together they represent a substantial reduction in risk.
Conclusion
How HPV causes cancer is a story of slow biological accumulation — a process that requires years, specific conditions, and multiple missed opportunities for detection. The mechanism is real and worth understanding, but so is the context: most HPV infections clear without intervention, the progression to cancer takes decades, and screening exists specifically to interrupt that progression at the pre-invasive stage.
Next Steps
- Schedule or confirm your screening. If you have a cervix and have not had a Pap smear or HPV co-test within the recommended interval, contact your healthcare provider. This is the single most effective action you can take.
- Know your HPV type. Not all HPV strains carry the same risk. Ask your provider whether your test result identifies the specific strain, and discuss what that means for your monitoring schedule.
- Stop smoking, if applicable. Smoking is the most consistently documented lifestyle co-factor for CIN progression. Cessation reduces that risk.
- Support your immune system actively. Adequate sleep, a nutrient-dense diet, stress management, and evidence-informed supplementation all contribute to immune competence — the primary mechanism by which HPV is cleared.
- Do not wait passively. If you have received a positive HPV result or an abnormal Pap finding, follow up with your provider rather than adopting a watch-and-wait approach without guidance.
Related Reading
- Can HPV turn into cancer? Understanding the real risk — a focused look at the statistical likelihood that a positive HPV result will progress.
- Why HPV doesn't clear in some people — the immunological and lifestyle factors that determine whether an infection becomes persistent.
- AHCC HPV success stories — accounts from individuals who used AHCC as part of their HPV management approach.
- The shocking truth about HPV and cervical cancer — a broader overview of the HPV-cervical cancer relationship and what the numbers actually mean.
References
- Centers for Disease Control and Prevention. Human Papillomavirus (HPV). https://www.cdc.gov/hpv
- World Health Organization. Human papillomavirus (HPV) and cervical cancer. https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer
- National Cancer Institute. HPV and Cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
- National Cancer Institute. Cervical Cancer Screening. https://www.cancer.gov/types/cervical/screening
- Doorbar J, et al. The biology and life-cycle of human papillomaviruses. Vaccine. 2012;30 Suppl 5:F55-70. https://pubmed.ncbi.nlm.nih.gov/23199966/
- Scheffner M, et al. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell. 1990;63(6):1129-1136.
- Dyson N, et al. The human papilloma virus-16 E7 oncoprotein is able to bind to the retinoblastoma gene product. Science. 1989;243(4893):934-937.
- Smith JA, et al. AHCC supplementation to support immune function to clear persistent human papillomavirus infections. Frontiers in Oncology. 2022. https://pubmed.ncbi.nlm.nih.gov/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







