


Most people who receive a positive HPV result walk away knowing only one thing: the virus is present. What they are rarely told — and what changes nearly everything about their clinical picture — is which HPV type they carry. Whether you were handed a result that said "high-risk HPV detected" with no further detail, or you received a specific number like HPV 16 or HPV 31 without understanding what it means, the gap between those two situations is clinically significant. Your HPV type determines your monitoring schedule, your realistic risk level, and how long clearance may reasonably take.
Key Takeaways
- Over 200 HPV types exist, but approximately 14 are classified as high-risk mucosal strains with documented links to cancer — and not all of those carry equal risk.
- Standard HPV co-tests detect high-risk HPV as a group; they often do not identify which specific strain is present.
- Current clinical guidelines treat HPV 16 and HPV 18 differently from other high-risk strains — a distinction that directly affects whether you are referred for colposcopy or simply asked to return in 12 months.
- HPV 16 is the most persistence-prone high-risk strain, which makes knowing whether you carry it especially relevant for monitoring timelines.
- If your result does not include genotype information, you can ask your provider to order a genotyping test — it is a reasonable and increasingly standard clinical request.
In This Article
The HPV Type Landscape
More than 200 distinct HPV types have been identified, and the vast majority of them never cause any health problem that a person would notice. Understanding how they are categorized helps clarify why some positive results are medically urgent and others are not.
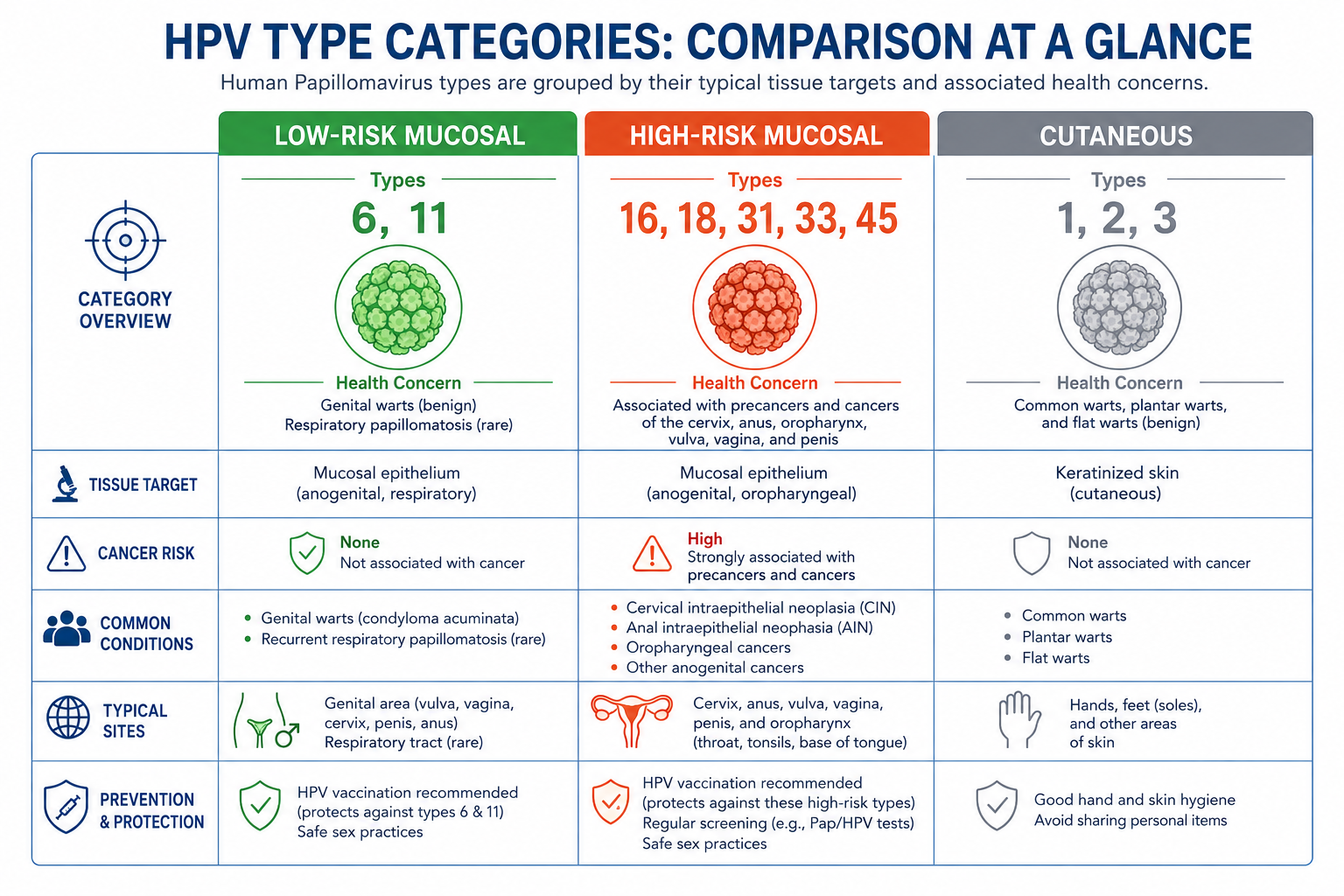
HPV types fall into three broad categories based on where they infect and what they can cause:
| Category | Common Examples | Primary Health Concern |
|---|---|---|
| Low-risk mucosal | 6, 11 | Genital warts — not associated with cancer |
| High-risk mucosal | 16, 18, 31, 33, 45, 52, 58, and others | Persistent infection can lead to cellular changes and cancer |
| Cutaneous | 1, 2, 3, 4, 10 | Common warts, plantar warts, flat warts — medically harmless |
The clinical conversation around HPV almost exclusively concerns mucosal HPV types — the strains that infect genital and oral tissues. Cutaneous types, while extremely common in both children and adults, are not the subject of cancer screening programs and are not what your gynecologist or primary care provider is testing for.
Within the mucosal category, approximately 14 strains are formally classified as high-risk by the International Agency for Research on Cancer (IARC). These are the strains that, when persistent, can drive the cellular changes that lead to cervical, oropharyngeal, anal, vulvar, vaginal, and penile cancers. According to the CDC HPV is responsible for nearly all cervical cancers and a significant proportion of other anogenital and oropharyngeal cancers.
Low-risk mucosal types — primarily HPV 6 and HPV 11 — cause approximately 90% of genital warts cases. They are not linked to cancer. A positive result for a low-risk type is not a cancer concern, though it may require treatment if warts are symptomatic.
Why Your Specific Type Matters
"HPV positive" without type information is an incomplete clinical picture — and that incompleteness has real consequences for the decisions that follow.
There are three reasons why knowing your specific HPV type is clinically meaningful:
1. Risk level is not uniform across types
Not all HPV types carry the same cancer risk. Low-risk and high-risk strains have fundamentally different implications. A person who tests positive for HPV 6 (low-risk) and a person who tests positive for HPV 16 (high-risk) are in entirely different clinical situations — but both results might be reported simply as "HPV positive" on a basic test. According to the National Cancer Institute, HPV 16 alone accounts for approximately 50% of cervical cancers globally. That is not a statistic that applies equally to all HPV types. For a deeper look at the cancer mechanism, the article on how HPV causes cancer explains the cellular pathway in detail.
2. Monitoring protocols differ by type
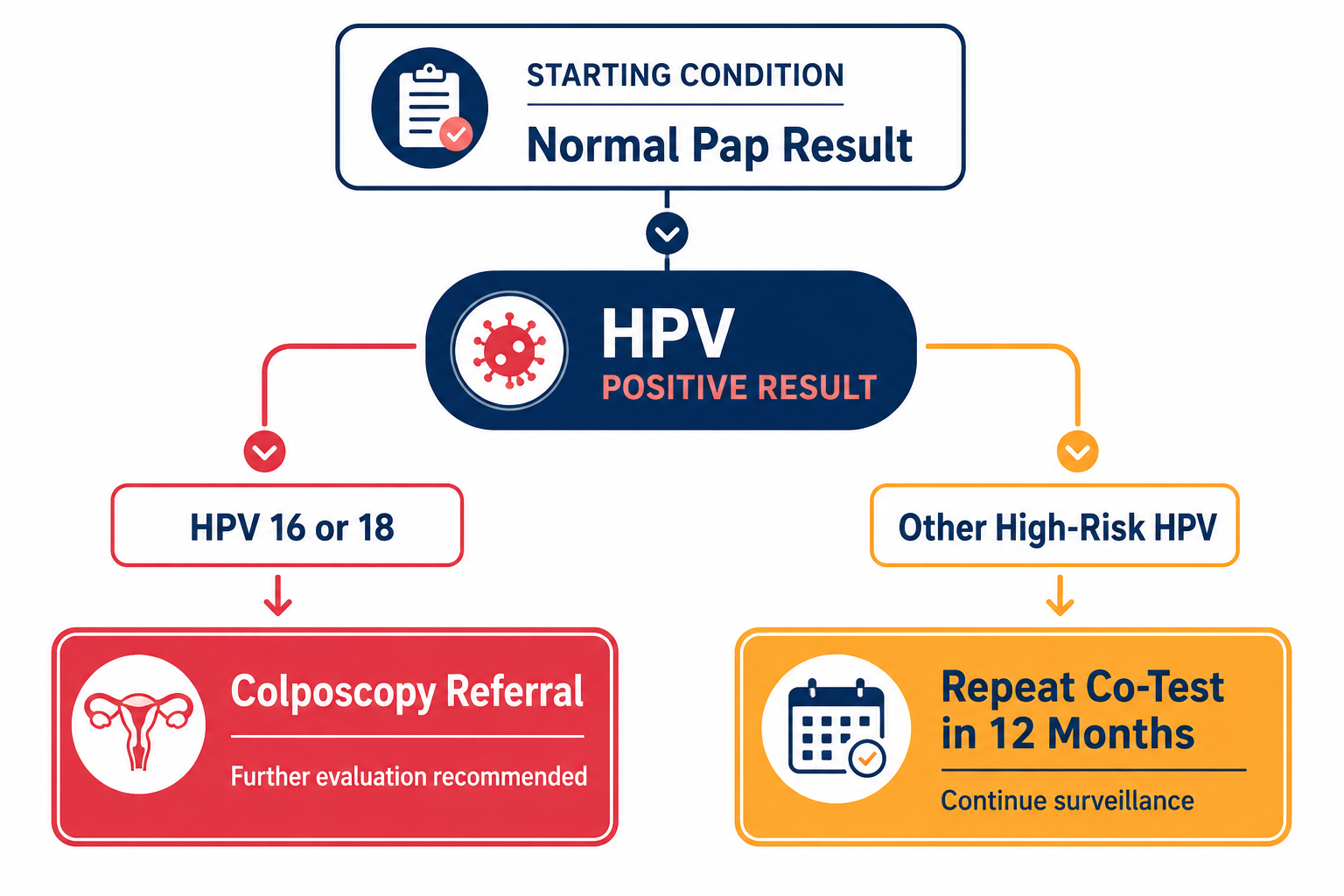
Current clinical guidelines from ASCCP and ACOG do not treat all high-risk HPV strains the same way. A person who tests positive for HPV 16 or HPV 18 with a normal Pap smear is typically referred for colposcopy. A person who tests positive for a different high-risk strain with a normal Pap is typically asked to return for a repeat co-test in 12 months. These are meaningfully different clinical responses — and the difference depends entirely on knowing which type is present. For a detailed breakdown of why HPV 16 and 18 specifically trigger more aggressive follow-up, the article on why HPV 16 and HPV 18 are the most dangerous strains covers this in depth.
3. Clearance timelines vary by type
High-risk strains — particularly HPV 16 — are more persistence-prone than low-risk strains or other high-risk types. Knowing your type helps set realistic expectations: if you carry HPV 16, you may need to monitor for longer before expecting a negative result. If you carry a low-risk type, clearance is typically faster and the follow-up less intensive.
Your HPV type is not a curiosity. It is clinically actionable information that shapes what happens next.
Standard HPV Tests vs Genotyping
Many patients do not realize that there are different levels of HPV testing — and that the level used in their case determines how much information they actually receive.
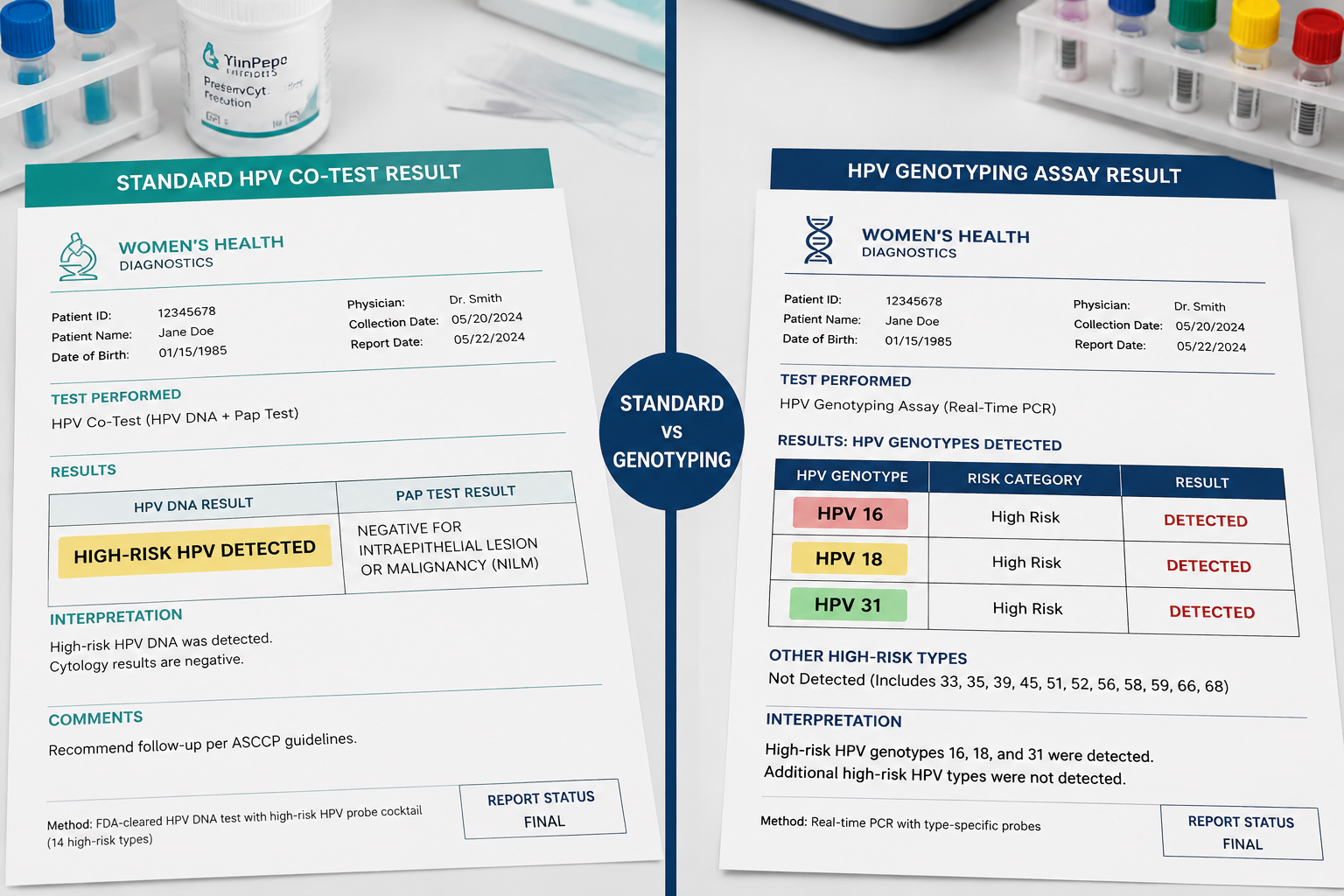
Standard HPV co-test (most common in routine screening): This test detects the presence of high-risk HPV strains as a group. The result is typically reported as "high-risk HPV detected" or "high-risk HPV not detected." It does not tell you which specific strain is present. This is what most routine Pap co-testing uses, and it is the reason many patients leave their appointment knowing they have high-risk HPV without knowing which one.
Genotyping tests: These tests can identify specific HPV strains. Different assays have different levels of specificity:
| Test | What It Identifies | Notes |
|---|---|---|
| Cobas HPV Test | HPV 16 individually, HPV 18 individually, other high-risk as a pooled group | Widely used in clinical settings |
| BD Onclarity HPV Assay | HPV 16, 18, 31, 45, 51, 52 individually; others pooled | First FDA-approved assay for self-collection (May 2024) |
| Aptima HPV Assay | Detects E6/E7 mRNA from high-risk strains — not genotype-specific | Measures active viral expression rather than presence alone |
Whether you received genotyping depends on which test your laboratory used and what your provider ordered — not all providers routinely request extended genotyping. If your result states only "high-risk HPV detected," you most likely had a standard pooled test. That does not mean your provider made an error; it means you may have grounds to ask for more specific information at your next visit.
For context on newer testing options, including self-collection, the article on self-sampling HPV tests explains how these methods work and whether they are appropriate for your situation.
What Your Result Actually Tells You
HPV results are reported in several different formats depending on the test used and the laboratory. Here is how to interpret the most common result language:
| Result Language | What It Means | What to Ask Your Provider |
|---|---|---|
| "HPV positive" | At least one HPV strain detected; type and risk category unknown | Ask for high-risk vs low-risk classification |
| "High-risk HPV detected" | A high-risk strain is present; specific type unknown | Ask whether genotyping was performed |
| "HPV 16 positive" | The highest-risk individual strain confirmed present | Ask about colposcopy referral |
| "HPV 18 positive" | Second highest-risk individual strain confirmed present | Ask about colposcopy referral |
| "HPV 16/18 negative, other high-risk positive" | A high-risk strain is present but not the two highest-risk types | Repeat co-test typically recommended in 12 months |
| "HPV negative" | No detected HPV, or below assay threshold | Continue standard screening schedule |
The most important distinction to clarify with your provider is whether your result is type-specific or pooled. A pooled "high-risk HPV detected" result leaves open the question of whether you carry HPV 16 or 18 — the two strains that trigger different clinical pathways — or one of the other high-risk types that carry lower but still real risk.
If you have received an HPV positive result alongside a normal Pap smear and are uncertain what it means for your follow-up schedule, the article on HPV positive but normal Pap addresses that specific scenario in detail.
How Monitoring Changes by Type
This is the section where the clinical importance of knowing your HPV type becomes most concrete. Current ASCCP 2019 Risk-Based Management Guidelines differentiate follow-up pathways based on HPV type and cytology result. The table below reflects general guideline frameworks — individual providers may vary their recommendations based on clinical judgment, patient history, and age.
| HPV Type | Cytology Result | Typical Guideline Pathway |
|---|---|---|
| HPV 16 or 18 | Normal (NILM) | Colposcopy referral |
| HPV 16 or 18 | Abnormal (ASCUS or higher) | Colposcopy referral |
| Other high-risk HPV | Normal (NILM) | Repeat co-test in 12 months |
| Other high-risk HPV | ASCUS | Colposcopy or repeat testing depending on age and history |
| Other high-risk HPV | LSIL or higher | Colposcopy referral |
| Low-risk HPV | Any | No cancer surveillance; wart management if symptomatic |
The table above illustrates exactly why knowing your specific HPV type matters: HPV 16 or 18 with a completely normal Pap smear triggers a colposcopy referral under current guidelines. Other high-risk strains with a normal Pap typically do not — they warrant watchful waiting with a repeat test in 12 months.
If you do not know your type, you cannot determine which of these pathways applies to you. A person with a pooled "high-risk HPV detected" result and a normal Pap is in a genuinely ambiguous position: they may be in the colposcopy pathway or the 12-month repeat pathway, and they cannot know which without type-specific information.
A note on clinical variation: Guidelines provide frameworks, not mandates. Your provider may recommend colposcopy even for non-16/18 high-risk strains based on your age, prior results, or other risk factors. The guidelines represent population-level risk thresholds — your individual clinical picture may differ.
How to Find Out Your HPV Type
If you do not currently know your HPV type, there are practical steps you can take to get that information.
Step 1: Review your lab report
If you have access to your test results through a patient portal or paper copy, look for specific genotype language. A result that states only "high-risk HPV detected" or "HPV positive" indicates a standard pooled test was used. A result that names a specific type — HPV 16, HPV 18, HPV 31 — indicates genotyping was performed.
Step 2: Call your provider's office directly
Ask specifically: "Did my HPV test include genotyping for HPV 16 and HPV 18?" If the answer is no, ask whether genotyping can be ordered with your next co-test. This is a reasonable clinical request, not an unusual one.
Step 3: Ask about coverage
Not all insurance plans cover extended genotyping as a standard offering, though it is increasingly part of routine practice in well-equipped laboratories. Your provider can advise on what is available and what your plan covers. In many cases, the additional cost is modest.
Step 4: Ask about self-collection options
The FDA approved self-collected HPV testing in clinical settings in May 2024 using the BD Onclarity assay, which includes extended genotyping for multiple individual strains. If your provider offers self-collection, this may be an option worth discussing. The article on self-sampling HPV tests provides a thorough overview of how these tests work and whether they are right for different situations.
The most important action is simply to ask. Many patients assume their provider has already given them all relevant information — but in a busy clinical setting, genotype specifics are not always communicated unless the patient asks directly.
Does HPV Type Affect Clearance?
Yes — with important caveats about what the research can and cannot tell us at an individual level.
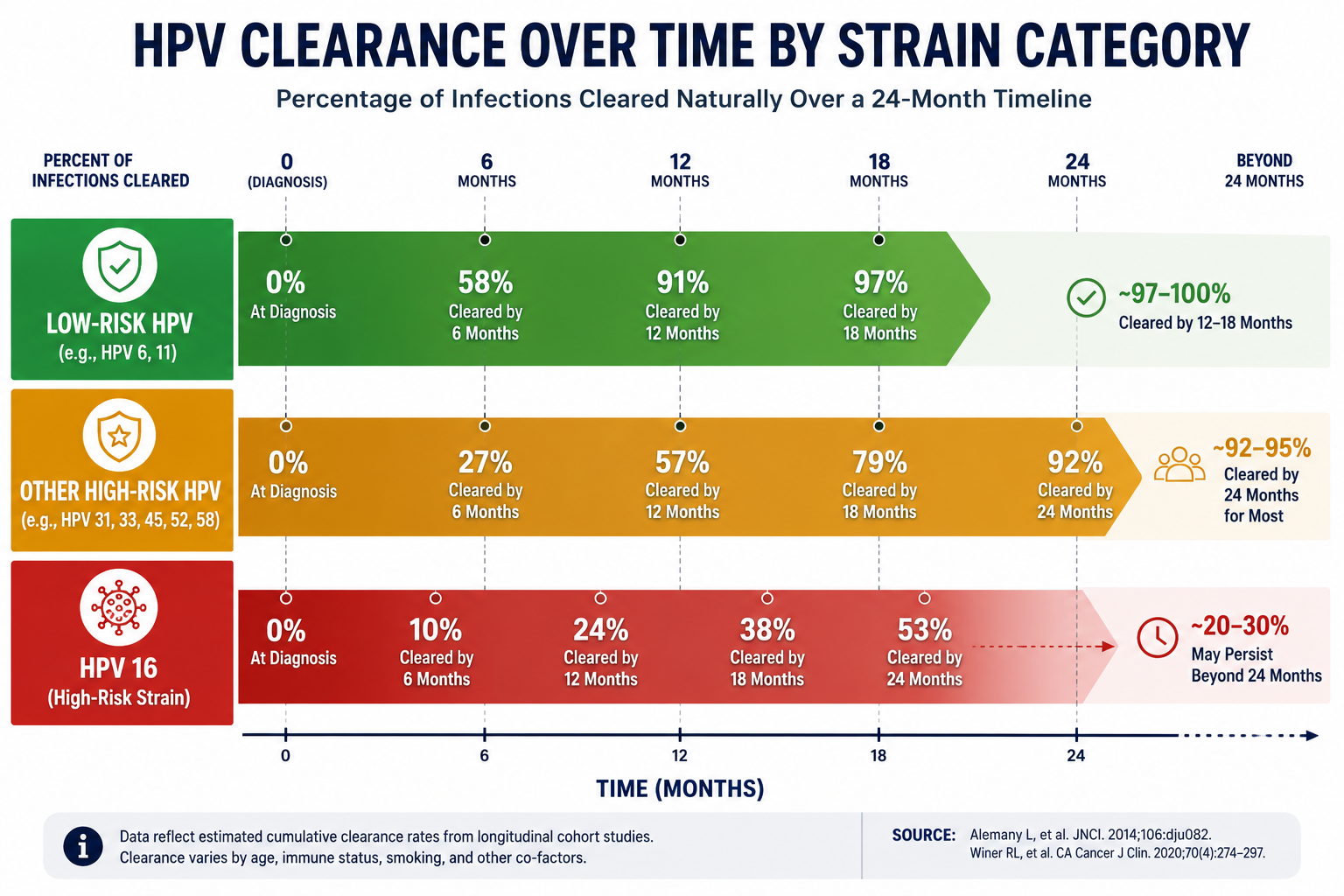
Low-risk strains (6, 11): These typically clear within 12 to 18 months in people with healthy immune function. Clearance rates are generally high, and the clinical concern is symptom management (genital warts) rather than cancer surveillance.
High-risk strains other than HPV 16: Overall clearance rates across high-risk HPV strains are approximately 90% within two years, consistent with CDC data on HPV natural history. Persistence is more common than with low-risk strains, but the majority of infections still resolve without intervention in immunocompetent individuals.
HPV 16 specifically: HPV 16 is the most persistence-prone of the high-risk strains. Studies consistently show that HPV 16 remains detectable longer than other high-risk types in a meaningful proportion of people. This is one reason why HPV 16 triggers more aggressive monitoring even when cytology is normal — not because clearance is impossible, but because the consequences of persistent HPV 16 are the most clinically significant of any individual strain.
Multiple concurrent strains: It is possible to carry more than one HPV type simultaneously. Clearing one strain does not automatically clear others. If you carry multiple types, a follow-up test may show partial clearance — one strain undetectable while another remains present. This is normal and does not indicate treatment failure.
These are population-level observations, not individual predictions. The immune system's ability to clear HPV depends on many factors beyond strain type — including smoking status, nutritional status, stress, sleep, and immune health. For a comprehensive look at why some infections persist longer than others, the article on why HPV doesn't clear in some people covers the full range of persistence factors.
Immune Support and HPV Type
There is no antiviral drug that directly targets HPV — regardless of which type you carry. Clearance depends entirely on the immune system recognizing and suppressing the infection. This means that the factors supporting immune function are relevant across all HPV types, not just specific ones.
The most impactful modifiable factors for HPV clearance include:
- Smoking cessation — smoking is consistently associated with HPV persistence and is the single most impactful behavioral change for people who smoke
- Vitamin D optimization — adequate vitamin D levels support immune surveillance; the NIH Office of Dietary Supplements provides guidance on optimal ranges
- Sleep quality — immune function is significantly impaired by chronic sleep deprivation
- Stress reduction — chronic stress suppresses the cellular immune responses involved in viral clearance
For people seeking a supplement with specific HPV-related evidence, AHCC (Active Hexose Correlated Compound) is currently the only supplement with a published, placebo-controlled human clinical trial targeting HPV clearance. The trial, conducted by Dr. Judith Smith at UT Health Science Center at Houston and published on PubMed, enrolled women with persistent high-risk HPV infections and showed statistically significant clearance compared to placebo. The research protocol used 3 grams per day taken on an empty stomach for a minimum of six months.
For those interested in this option, NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility. At the research-validated dose of 3 grams per day, this corresponds to approximately four to five capsules daily.
One important transparency note: the published AHCC research does not stratify results by specific HPV type. The evidence base does not currently allow a claim that AHCC works better or worse for HPV 16 versus other high-risk strains. What the trial demonstrated is clearance across persistent high-risk HPV infections broadly — which is the population most people reading this article belong to.
For a thorough review of the evidence, the article on whether AHCC really helps clear HPV covers the published research, its limitations, and what it realistically means for someone in your situation.
This information is preliminary. AHCC is not FDA-approved as a treatment for HPV and should not be substituted for clinical monitoring or medical care.
Frequently Asked Questions
Does my doctor automatically test for my specific HPV type?
Not necessarily. Standard HPV co-tests used in routine Pap screening detect high-risk HPV as a group and report only "detected" or "not detected" without identifying the specific strain. Whether your test included genotyping depends on which assay your laboratory used and what your provider ordered. If your result does not name a specific type, it is reasonable to ask your provider whether genotyping was performed and whether it can be ordered at your next visit.
Is HPV 16 always more dangerous than other strains?
HPV 16 carries the strongest individual association with cancer — it accounts for approximately 50% of cervical cancers globally and is the dominant strain in HPV-related oropharyngeal cancers. However, "more dangerous" requires context. All high-risk strains carry real risk when persistent; the difference is one of degree and probability, not a categorical distinction between safe and unsafe. Other high-risk strains including 18, 31, 33, and 45 also have documented cancer associations. HPV 16 triggers more aggressive monitoring because the consequences of persistent infection are statistically the most significant — not because other high-risk strains are harmless.
Can I have more than one HPV type at the same time?
Yes. Co-infection with multiple HPV types is common, particularly in people who have had more than one sexual partner. A genotyping test may identify multiple strains simultaneously. Carrying multiple types does not automatically increase cancer risk in a simple additive way, but it does mean that follow-up testing may show partial clearance — one strain resolving while another remains detectable. Your provider will interpret results in the context of your full clinical picture.
My result says "high-risk HPV detected" — how do I find out which type?
Start by reviewing your lab report for any genotype-specific language. If none is present, call your provider's office and ask directly: "Was my HPV test genotyped for HPV 16 and HPV 18 specifically?" If the answer is no, ask whether a genotyping test can be ordered with your next co-test. This is a clinically reasonable request. At your next scheduled screening, a genotyping assay can provide the strain-specific information that a standard pooled test does not.
Does AHCC work differently for different HPV types?
The published clinical research on AHCC and HPV does not stratify results by specific HPV type, so there is no evidence base from which to say whether AHCC performs differently for HPV 16 versus HPV 31 or any other specific strain. The published trial enrolled women with persistent high-risk HPV broadly and showed clearance benefit compared to placebo across that group. Until type-stratified data is available, the honest answer is: we do not know whether type matters for AHCC response. What is known is that the trial population — persistent high-risk HPV — overlaps substantially with the population most concerned about their specific strain.
Conclusion
Receiving an HPV positive result without knowing which type you carry is more common than it should be. The distinction between a pooled "high-risk HPV detected" result and a type-specific result is not a minor detail — it determines your monitoring pathway, shapes your realistic risk picture, and sets appropriate expectations for clearance timelines.
Actionable next steps:
- Review your existing lab report. Look for genotype-specific language. If you see only "high-risk HPV detected," you received a standard pooled test.
- Contact your provider's office. Ask specifically whether your test included genotyping for HPV 16 and HPV 18. If not, request that genotyping be ordered at your next co-test.
- Understand your monitoring pathway. Once you know your type, confirm with your provider which follow-up schedule applies to you — colposcopy referral or repeat co-test in 12 months.
- Address the modifiable factors. Smoking cessation, vitamin D optimization, adequate sleep, and stress management are the most evidence-supported actions for supporting immune clearance — regardless of HPV type.
- Consider immune support with evidence behind it. If you are managing a persistent high-risk HPV infection and want a supplement with published clinical data, discuss AHCC with your provider. Review the evidence at does AHCC really help clear HPV before making a decision.
The most important step is the simplest: ask your provider which HPV type you have. That single piece of information changes the entire conversation about what comes next.
Related Reading
- Why HPV 16 and HPV 18 Are the Most Dangerous HPV Strains — A detailed look at why these two strains trigger different clinical responses and carry the strongest cancer associations.
- HPV Positive but Normal Pap — What Does It Mean? — Explains the clinical significance of this common result combination and what follow-up typically looks like.
- Why HPV Doesn't Clear in Some People — Covers the full range of factors that contribute to HPV persistence beyond strain type alone.
- I Have HPV — Now What? 8 Steps to Clear the Virus Naturally — A practical action plan for people recently diagnosed, covering lifestyle, monitoring, and immune support options.
References
- Centers for Disease Control and Prevention. HPV Fact Sheet. https://www.cdc.gov/hpv
- ASCCP. 2019 ASCCP Risk-Based Management Consensus Guidelines. https://www.asccp.org/management-guidelines
- National Cancer Institute. HPV and Cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
- NIH Office of Dietary Supplements. Vitamin D Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- PubMed — AHCC Clinical Research Database. https://pubmed.ncbi.nlm.nih.gov/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







