


Most people with HPV are told it clears on its own within two years — and for the majority, it does. If you are reading this, you are likely not in that majority. Whether your HPV has been persistently positive for over a year despite lifestyle changes, or it appeared to clear and then returned on a subsequent test, you are dealing with a clinically distinct situation that demands a more rigorous look at the evidence. This article reviews the best supplements for recurrent HPV based on published research — not general immune support claims, but studies specifically involving HPV-positive participants. The goal is an honest, tiered assessment of what the evidence actually shows, including where it is strong, where it is preliminary, and where it is essentially absent.
Key Takeaways
- AHCC is the only supplement with a published, placebo-controlled human trial specifically targeting HPV clearance — making it the highest-evidence option currently available.
- The combination of EGCG, folate, vitamin B12, and hyaluronic acid has multiple clinical studies supporting HPV clearance and cervical lesion improvement, representing the strongest emerging evidence outside of AHCC.
- Vitamin D and folate deficiencies are independently associated with HPV persistence — correcting them is low-cost, low-risk, and mechanistically sound.
- Echinacea has randomized evidence specifically for low-risk HPV wart recurrence, but this evidence does not extend to high-risk HPV clearance.
- No supplement has been approved by the FDA to treat, cure, or prevent HPV — the evidence reviewed here is preliminary and should be discussed with a qualified healthcare provider.
In This Article
- Recurrent vs persistent HPV — what you're actually dealing with
- How to evaluate supplement evidence
- AHCC — the strongest HPV-specific human trial evidence
- EGCG + Folate + B12 + Hyaluronic Acid — emerging combination evidence
- DIM and Indole-3-Carbinol — cervical lesion support
- Vitamin D — correcting the most common deficiency
- Folate — the overlooked foundational supplement
- Echinacea — evidence for wart recurrence specifically
- Evidence comparison summary
- Can these supplements be combined?
- Frequently asked questions
Recurrent vs Persistent HPV — What You're Actually Dealing With
Before evaluating any supplement, it is worth being precise about terminology — because "recurrent HPV" can describe two clinically different situations, and the distinction affects which approach makes the most sense.
Persistent HPV is the more common scenario among readers of this article. The same strain has been detectable for 12 months or longer without clearing. The immune system has not successfully suppressed the virus, and the standard "watch and wait" approach has not produced a negative result. This is not a failure of patience — it is a sign that something in the immune response to this specific virus is not functioning optimally.
Recurrent HPV after apparent clearance is a different scenario. The virus appeared to clear — a subsequent test came back negative — and then a later test returned positive again. Two explanations are possible. The first is reactivation: the virus entered a latent state but was never fully eliminated. During a period of immune suppression — from stress, illness, poor sleep, or other factors — the virus reactivated to detectable levels. The second is re-infection through new sexual exposure. There is currently no clinical test that can distinguish these two scenarios. This distinction matters for strategy: if reactivation is likely, immune support becomes the central focus; if re-infection is more plausible given circumstances, barrier protection alongside immune support becomes equally relevant.
For a detailed look at the biological and lifestyle factors that determine why some people clear HPV and others do not, the analysis at why some people clear HPV faster than others covers the immune mechanisms in depth.
How to Evaluate Supplement Evidence
The supplement market for HPV is crowded with products making broad immune support claims. Very few have any human clinical evidence. Fewer still have evidence specifically involving HPV-positive participants. To evaluate the supplements reviewed in this article consistently, the following evidence framework applies:
| Evidence Tier | Definition | What It Means |
|---|---|---|
| Tier 1 | Randomized, placebo-controlled human trial | Strongest evidence; can establish causation |
| Tier 2 | Non-randomized clinical studies or case series | Promising; cannot establish causation alone |
| Tier 3 | In vitro (lab) or animal studies only | Mechanistic rationale; no human evidence |
| No evidence | Marketing claims only | Cannot be evaluated scientifically |
A 2023 review published in PMC (PMC10056139) systematically assessed natural compounds for HPV persistence prevention and found that only a small number had any meaningful human clinical data. That finding shapes the honest assessment that follows.
AHCC — The Strongest HPV-Specific Human Trial Evidence
Evidence tier: Tier 1 (one published Phase II randomized, placebo-controlled trial)
AHCC (Active Hexose Correlated Compound) is a standardized extract derived from the mycelia of shiitake mushrooms. Its primary bioactive compounds are alpha-glucans, which have been studied for their effects on immune cell activity — specifically natural killer (NK) cells, dendritic cells, and T-cell populations involved in viral clearance.
The most significant evidence comes from a Phase II randomized, double-blind, placebo-controlled trial conducted by Dr. Judith Smith at the UT Health Science Center at Houston. Women with persistent high-risk HPV received 3 grams of AHCC daily in a fasted state over six months. The trial showed statistically significant HPV clearance in the AHCC group compared to placebo, and clearance was sustained at follow-up testing. This is the only supplement reviewed in this article with this level of HPV-specific human trial evidence. A broader review of medicinal mushroom compounds in HPV management, published in 2025, further contextualizes AHCC's position within the research landscape (PMC12300315).
Important limitations: This is one trial. Replication in larger, independent studies is needed before drawing firm conclusions. Not every participant in the trial responded. AHCC is not FDA-approved as an HPV treatment. The evidence is promising and preliminary — not definitive.
Protocol: The trial used 3 grams per day, taken on an empty stomach, for a minimum of six months. For persistent high-risk cases, some practitioners extend this to nine to twelve months. NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility — reaching the 3-gram clinical dose requires approximately four to five capsules daily. For a full review of the trial evidence, see does AHCC really help clear HPV. For protocol specifics, the AHCC dosage guide for HPV covers clinical study findings in detail. Research on AHCC across multiple conditions is indexed at PubMed.
EGCG + Folate + B12 + Hyaluronic Acid — Emerging Combination Evidence
Evidence tier: Tier 2 (multiple non-randomized clinical studies)
This combination represents the most substantive emerging evidence base for HPV supplements outside of AHCC — and it is largely absent from mainstream HPV supplement content. The formula consists of epigallocatechin gallate (EGCG) from green tea extract, folic acid, vitamin B12, and hyaluronic acid. The evidence is for this combination as a formula, not for each ingredient in isolation.
The published evidence includes:
- Aragona et al.: 17 of 20 patients with HPV infection showed complete viral clearance following treatment with this combination formula.
- Tinelli et al.: 86 patients treated orally with the combination showed HPV clearance at three months compared to an untreated control group. Cervical lesions improved in the treated group, while the control group showed some progression toward high-grade squamous intraepithelial lesions (HSIL).
- 2024 clinical study (PMC12155352): 106 HPV-positive patients received EGCG 200 mg, folate 400 mcg, B12 1 mg, and hyaluronic acid 50 mg daily for six months. Results showed improvement in HPV clearance rates and reduction of cervical lesions (PMC12155352).
- The 2023 PMC systematic review referenced above identified this combination as having the most consistent clinical evidence of any natural supplement combination for HPV.
Why EGCG specifically matters: Laboratory research shows that EGCG may suppress HPV E6 and E7 oncoproteins — the viral proteins responsible for disrupting normal cell cycle regulation and driving progression toward dysplasia. This gives the combination a mechanistic rationale beyond general immune support, which is particularly relevant for high-risk HPV strains.
Limitations: The studies are smaller, non-randomized, and have emerged primarily from a limited number of research groups. A placebo-controlled trial of the same rigor as the Smith et al. AHCC study has not yet been published for this combination. This combination is not FDA-approved as an HPV treatment.
Availability: This combination is not a NovaHerbs product. The studied formula — EGCG, folate, B12, and hyaluronic acid — can be assembled from individual supplements available at pharmacies and health stores. Specific brand recommendations are outside the scope of this article; discuss sourcing with a healthcare provider or pharmacist.
DIM and Indole-3-Carbinol — Cervical Lesion Support
Evidence tier: Tier 2-3 (observational and in vitro data)
DIM (diindylmethane) is a metabolite of indole-3-carbinol (I3C), a compound found naturally in cruciferous vegetables such as broccoli, cauliflower, and Brussels sprouts. Both compounds have been studied in the context of cervical health, primarily through their effects on estrogen metabolism.
The proposed mechanism involves shifting estrogen metabolism toward less cancer-promoting pathways — specifically increasing the ratio of 2-hydroxyestrone to 16-alpha-hydroxyestrone. Some observational studies suggest that this shift may support cervical lesion regression in CIN 1 and CIN 2 cases. DIM also has antioxidant properties that may reduce oxidative stress in cervical tissue, which is elevated in the context of persistent HPV infection.
What the evidence does not show: There is no published, placebo-controlled trial demonstrating that DIM or I3C independently clears HPV infection. The evidence is mechanistically interesting and observationally suggestive — not confirmatory.
Best fit: DIM may be most relevant for individuals who have both HPV and cervical intraepithelial neoplasia (CIN), particularly those with hormonal considerations. It is generally well tolerated at standard doses. Anyone taking hormonal medications — including oral contraceptives — should discuss DIM supplementation with their prescribing provider before use, as estrogen metabolism modulation may interact with these medications.
Vitamin D — Correcting the Most Common Deficiency
Evidence tier: Tier 2 for immune function; Tier 3 for HPV-specific clearance
Vitamin D is not being presented here as an HPV treatment. It is being presented as a deficiency correction strategy with strong mechanistic rationale for immune function. Vitamin D deficiency is widespread — particularly in northern latitudes, during winter months, and among people with limited sun exposure — and it is directly associated with impaired T-cell and natural killer (NK) cell function. These are the exact immune cells involved in HPV clearance.
Observational studies have found associations between low serum 25(OH)D levels and higher rates of HPV persistence. The NIH Vitamin D fact sheet identifies immune modulation as one of vitamin D's established physiological roles.
Practical approach: Test your serum 25(OH)D level through a standard blood panel. A target range of 40–60 ng/mL is generally associated with optimal immune function. Supplement to correct deficiency, particularly through winter months when dietary and sun-derived vitamin D is insufficient. This is not a claim that vitamin D supplementation clears HPV — it is a claim that correcting a deficiency that may be impairing immune function is a reasonable, evidence-supported step.
Folate — The Overlooked Foundational Supplement
Evidence tier: Tier 2 (observational research)
Low folate levels have been associated with HPV persistence and higher rates of cervical dysplasia in multiple observational studies. Folate is essential for DNA repair and methylation — processes that are disrupted by persistent HPV infection, particularly in cervical epithelial cells. It is also one of the four components in the EGCG combination formula reviewed above, which suggests it may contribute to that formula's observed effects.
Practical approach: Assess dietary folate intake first. Dark leafy greens, lentils, chickpeas, and fortified grains are key sources. For supplementation, methylfolate (5-MTHF) is the active form and is preferable — particularly for individuals with MTHFR genetic variants that impair the conversion of folic acid to its active metabolite. Standard supplementation at 400–800 mcg daily is inexpensive and carries minimal risk at recommended doses.
The NIH Folate fact sheet provides a thorough overview of folate's role in cellular health and DNA integrity. This is a low-cost, low-risk foundational supplement worth taking regardless of other supplement decisions — particularly for anyone whose diet is low in leafy vegetables.
Echinacea — Evidence for Wart Recurrence Specifically
Evidence tier: Tier 2, narrow scope
Echinacea requires precise framing because the evidence is real but narrow. One prospective randomized study (PMC6487159) examined Echinacea angustifolia and E. purpurea specifically for the recurrence of genital condylomatosis — warts caused by low-risk HPV strains 6 and 11 — following standard wart treatment. When Echinacea was combined with hyaluronic acid, results showed a meaningful reduction in wart recurrence compared to controls.
The critical scope limitation: This evidence applies specifically to low-risk HPV wart recurrence. It does not apply to high-risk HPV clearance, and it does not address cancer prevention. For readers whose recurrent HPV involves genital warts caused by low-risk strains, this evidence is directly relevant. For readers with persistent high-risk HPV (strains 16, 18, 31, 33, 45, and others), the Echinacea evidence does not directly address their situation.
This distinction is not a minor caveat — it determines whether Echinacea belongs in a given individual's protocol at all. Applying low-risk HPV wart evidence to high-risk HPV management is a category error that appears frequently in supplement content.
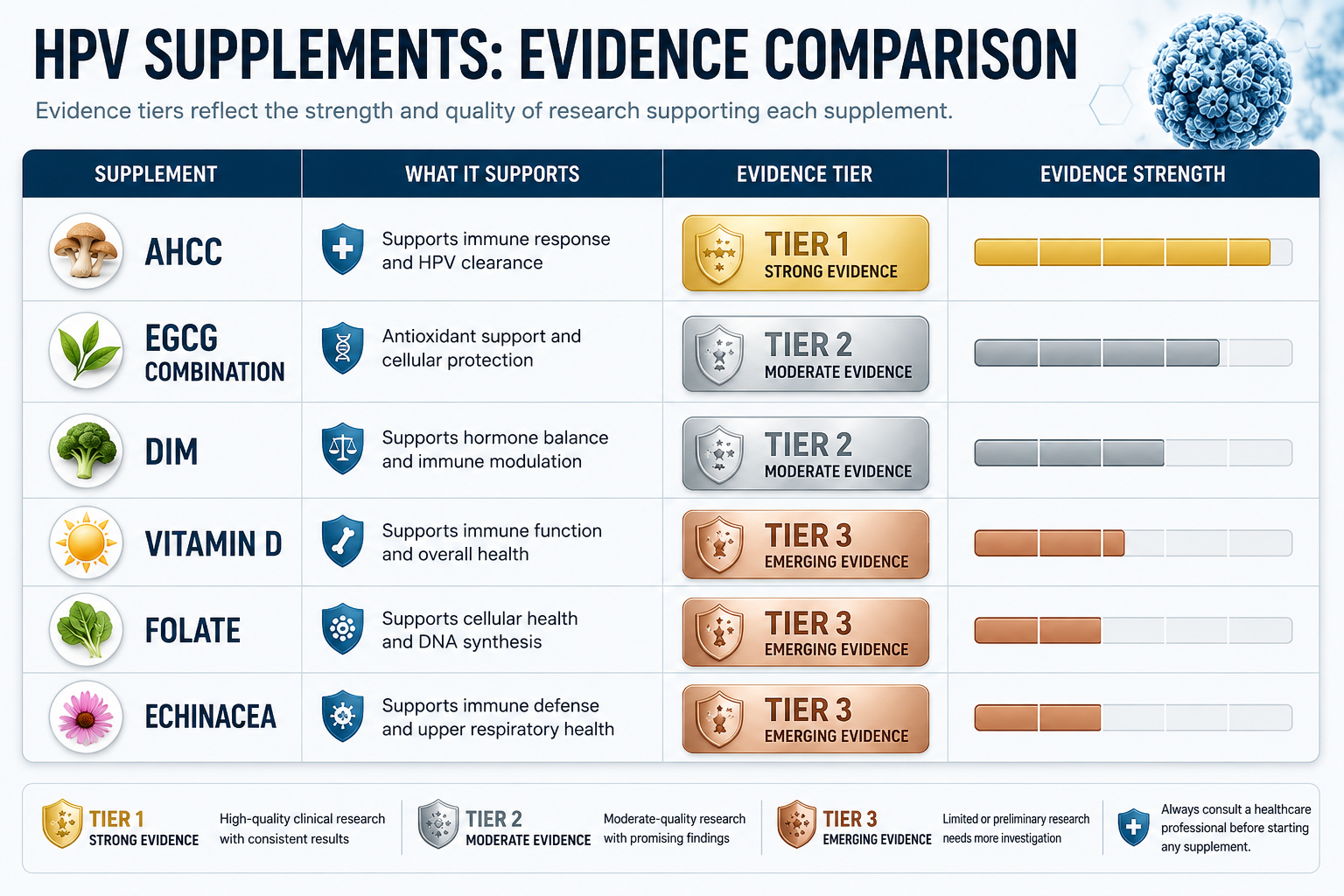
Evidence Comparison Summary
The table below summarizes the evidence quality for each supplement reviewed in this article. This is the reference point for making an informed protocol decision.
| Supplement | Evidence Tier | HPV-Specific Human Evidence | Best Evidence For | Key Limitations |
|---|---|---|---|---|
| AHCC | Tier 1 | Phase II RCT (Smith et al.) | Persistent high-risk HPV clearance | One trial; not everyone responds |
| EGCG + Folate + B12 + HA | Tier 2 | Multiple clinical studies (Aragona, Tinelli, 2024) | HPV clearance and CIN lesion improvement | Non-randomized; smaller studies |
| DIM / I3C | Tier 2-3 | Observational and mechanistic | CIN support; estrogen metabolism | No HPV clearance RCT |
| Vitamin D | Tier 2 (immune) | Observational association with persistence | Correcting immune deficiency | Not HPV-specific treatment |
| Folate | Tier 2 | Observational association | Deficiency correction; part of EGCG combo | Not standalone HPV treatment |
| Echinacea | Tier 2, narrow | Randomized study (wart recurrence only) | Low-risk HPV wart recurrence | Not applicable to high-risk HPV |
No supplement in this table has been approved by the FDA to treat or prevent HPV. Evidence quality varies considerably, and individual responses will differ. This table is a tool for informed conversation with a healthcare provider — not a prescription.
Can These Supplements Be Combined?
Combining supplements is a common approach among people with persistent or recurrent HPV, and some combinations are more rational than others based on available evidence.
AHCC + Vitamin D + Folate: No known interactions exist among these three. This combination covers the supplement with the strongest HPV trial evidence (AHCC) plus two evidence-based deficiency corrections (vitamin D and folate). For most people, this represents a practical and manageable starting protocol. For broader lifestyle strategies that complement supplementation, the natural HPV clearance guide covers diet, sleep, and immune optimization in detail.
AHCC + EGCG combination: These two approaches are theoretically complementary — AHCC operates primarily through immune modulation, while EGCG is proposed to act through direct HPV oncogene suppression. No published trial has examined them together, and additive benefit has not been confirmed. Some practitioners use both simultaneously in persistent high-risk cases; this is a reasonable hypothesis but remains unvalidated.
Key practical notes for combining:
- AHCC must be taken in a fasted state for optimal absorption. Most other supplements reviewed here can be taken with food.
- Fat-soluble vitamins — including vitamin D — require dietary fat for absorption. Take them with a meal, not alongside fasted AHCC.
- If taking prescription medications, discuss any new supplement combination with your prescribing provider before starting.
An honest note on complexity: Combining multiple supplements increases both cost and protocol complexity. For most people, prioritizing the highest-evidence option — AHCC — with deficiency correction (vitamin D and folate) is a more practical and sustainable starting point than attempting a complex multi-supplement protocol simultaneously. For questions about AHCC timing, the article on why taking AHCC on an empty stomach matters explains the pharmacokinetic rationale.
Frequently Asked Questions
If AHCC didn't work the first time, should I try it again?
This is one of the most common questions from people with persistent HPV, and it deserves a direct answer. Protocol adherence is the first variable to assess — the clinical trial used 3 grams per day in a fasted state for six months, and deviations from this protocol (lower dose, taken with food, shorter duration) may reduce effectiveness. Before concluding that AHCC is not effective for a given individual, it is worth reviewing whether the protocol was followed precisely. The article the real reasons AHCC didn't work covers the most common protocol errors in detail. If the full protocol was followed correctly and no clearance occurred, adding the EGCG combination or addressing vitamin D and folate deficiencies may be worth discussing with a healthcare provider.
Is the EGCG/folate/B12/hyaluronic acid combination available as a single supplement?
The combination studied in the Italian clinical research (Aragona, Tinelli) was examined as a proprietary formula. The individual components — EGCG, methylfolate, B12, and hyaluronic acid — are available separately at pharmacies and health stores and can be assembled into a similar protocol. The studied doses were EGCG 200 mg, folate 400 mcg, B12 1 mg, and hyaluronic acid 50 mg daily. A healthcare provider or pharmacist can assist in sourcing appropriate individual supplements and confirming appropriate doses for a given individual's situation.
Can I take DIM and AHCC at the same time?
No known pharmacological interactions exist between DIM and AHCC. They operate through different proposed mechanisms — AHCC through immune modulation and DIM through estrogen metabolism. Taking them together is not contraindicated based on current evidence, but it adds cost and protocol complexity without confirmed additive benefit. For individuals with both persistent HPV and CIN lesions, the combination may be worth discussing with a gynecologist or integrative medicine provider who can assess individual hormonal and immune factors.
Does vitamin D directly clear HPV?
No. Vitamin D supplementation has not been shown in a controlled trial to directly clear HPV infection. What the evidence does support is that vitamin D deficiency impairs the T-cell and NK cell responses that are central to viral clearance — and that correcting this deficiency may restore immune function that is currently suboptimal. The distinction matters: vitamin D is not an antiviral agent, but it may be removing a barrier to the immune response that is supposed to be clearing the virus. Testing serum 25(OH)D levels is the appropriate first step before supplementing.
How long should I try any supplement before concluding it isn't working?
HPV clearance, when it occurs with supplementation, is typically assessed over a minimum of six months — which is the duration used in the Smith et al. AHCC trial. Testing too early (at three months or less) may not reflect the full immune response. A reasonable approach is to commit to a well-structured protocol for six months, then retest with the same HPV test type used previously. If no change is observed at six months, reassess protocol adherence, consider adding deficiency corrections, and discuss with a healthcare provider whether additional workup (immune panel, MTHFR testing, vitamin D levels) might reveal correctable factors.
Conclusion
Recurrent or persistent HPV is a legitimate clinical challenge that deserves more than generic immune support advice. The best supplements for recurrent HPV are those with actual human clinical evidence in HPV-positive populations — and that evidence landscape, while limited, does exist.
Actionable next steps:
- Start with the highest-evidence option. AHCC at 3 grams per day, taken fasted, for a minimum of six months represents the most evidence-supported supplement protocol currently available for persistent high-risk HPV.
- Test for deficiencies before supplementing broadly. A serum 25(OH)D test and a dietary assessment for folate intake are inexpensive first steps. Correcting deficiencies that may be impairing immune function is logical and low-risk.
- Consider the EGCG combination for cervical lesion concerns. If persistent HPV is accompanied by CIN, the EGCG + folate + B12 + hyaluronic acid combination has the most published clinical evidence of any natural supplement combination outside of AHCC. Discuss with your gynecologist.
- Match Echinacea evidence to your specific HPV type. If your recurrent HPV involves low-risk strains causing warts, Echinacea has relevant randomized evidence. If your concern is high-risk HPV, the evidence does not apply.
- Keep monitoring. No supplement replaces regular HPV testing and cervical screening. Continue scheduled follow-up appointments regardless of supplement use, and report any changes in test results to your healthcare provider.
Related Reading
- Why some people clear HPV faster than others — and what determines immune response
- Can HPV come back after clearance? What the science actually shows
- The real reasons AHCC didn't work — protocol errors and what to do next
- Best supplement for persistent HPV — a focused evidence review
- How to clear HPV naturally — lifestyle factors that support immune clearance
References
- Smith JA et al. AHCC supplementation and HPV clearance — Phase II randomized controlled trial. Available via PubMed: https://pubmed.ncbi.nlm.nih.gov/
- Aragona et al. / Tinelli et al. EGCG combination HPV studies. Referenced in: PMC12155352. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12155352/
- Preventing persistence of HPV with natural molecules — systematic review (2023). PMC10056139. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10056139/
- Medicinal mushrooms, probiotics and combinations in HPV management (2025). PMC12300315. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12300315/
- Echinacea and recurrence of genital condylomatosis — prospective randomized study. PMC6487159. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6487159/
- CDC HPV fact sheet. https://www.cdc.gov/hpv
- NIH Office of Dietary Supplements — Vitamin D fact sheet. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- NIH Office of Dietary Supplements — Folate fact sheet. https://ods.od.nih.gov/factsheets/Folate-HealthProfessional/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







