


Most HPV content is written for a 27-year-old. She gets a positive result, her doctor tells her the immune system usually clears the virus within one to two years, and that reassurance is largely accurate for her age group. But if you are sitting with a persistent HPV result at 52 — or 56, or 61 — that same reassurance does not fully apply to you, and most of what you find online will not tell you that directly.
HPV after 50 operates under a different set of biological rules. The immune system changes with age in ways that are well-documented and clinically significant. Menopause alters the local immune environment of the cervix. And the standard "watch and wait" guidance, while medically appropriate, can feel profoundly inadequate when you understand that the biological tailwind younger women rely on is no longer working in your favor at the same speed.
This article is the resource that should exist for women over 50 navigating a persistent HPV diagnosis — written plainly, without false reassurance, and with a clear focus on what you can actually do.
Key Takeaways
- The immune system's ability to clear HPV declines measurably after 50 due to a process called immune senescence — this is biology, not failure.
- Menopause reduces estrogen-dependent mucosal immunity in the cervix, making local HPV defense less effective.
- "Watch and wait" is not wrong, but for women over 50, combining monitoring with active immune support is a more complete strategy.
- Vitamin D deficiency, poor sleep, and chronic stress each independently suppress immune function — and all three are more common after 50.
- AHCC is the only supplement with a published, placebo-controlled human trial targeting HPV clearance; it warrants serious consideration as part of a broader immune support protocol.
In This Article
- How the immune system changes after 50
- The menopause factor
- Why "watch and wait" lands differently at 50
- How screening changes after menopause
- What you can actually do
- AHCC and immune support after 50
- Vitamin D — the most common deficiency
- Sleep and stress at 50
- Monitoring — what to expect
- Frequently asked questions
How the Immune System Changes After 50
The immune system does not fail at 50. It changes — gradually, measurably, and in ways that have direct consequences for how the body handles a persistent viral infection like HPV.
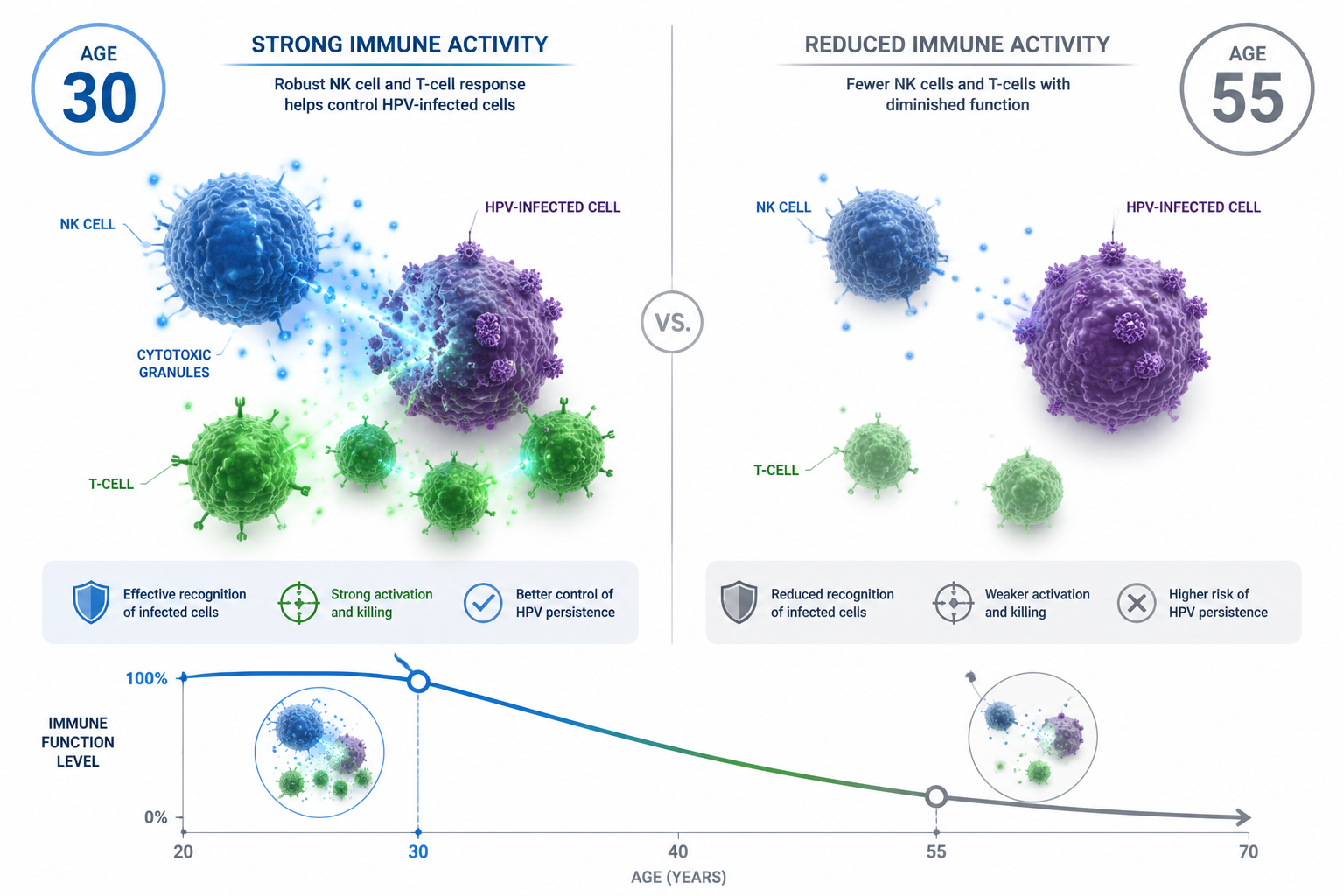
The process is called immune senescence: the age-related decline in immune function that affects both the speed and precision of the immune response. Research published through the NIH documents this process in detail. Two changes are particularly relevant to HPV clearance.
Natural killer (NK) cell activity declines. NK cells are part of the innate immune system — the body's first line of defense against virus-infected cells. They do not need prior exposure to a pathogen to act; they recognize and destroy abnormal cells on contact. After 50, NK cell activity decreases in both quantity and functional capacity. This matters for HPV because NK cells are among the primary immune actors targeting HPV-infected cervical cells.
T-cell precision diminishes. The adaptive immune system — which mounts a targeted response to specific pathogens — relies on T-cells to recognize and eliminate HPV-infected cells. With age, the diversity of the T-cell repertoire narrows, and the speed of the adaptive response slows. The immune system can still respond to HPV; it simply does so less efficiently and at a lower baseline level.
The practical consequence: an HPV infection that a 28-year-old's immune system might resolve in 12 to 18 months can persist for years in a 52-year-old — not because the infection is more aggressive, but because the immune response is operating at a reduced capacity. Understanding why HPV fails to clear in some people requires looking at both the virus and the immune environment — and after 50, the immune environment is a significant part of the answer.
This is not a reason for despair. It is a reason to be more deliberate about supporting immune function rather than relying on passive clearance.
The Menopause Factor
Immune senescence is a systemic process. Menopause adds a second, more localized layer of immune change that is specific to the cervix — and it is one that most HPV content does not address at all.
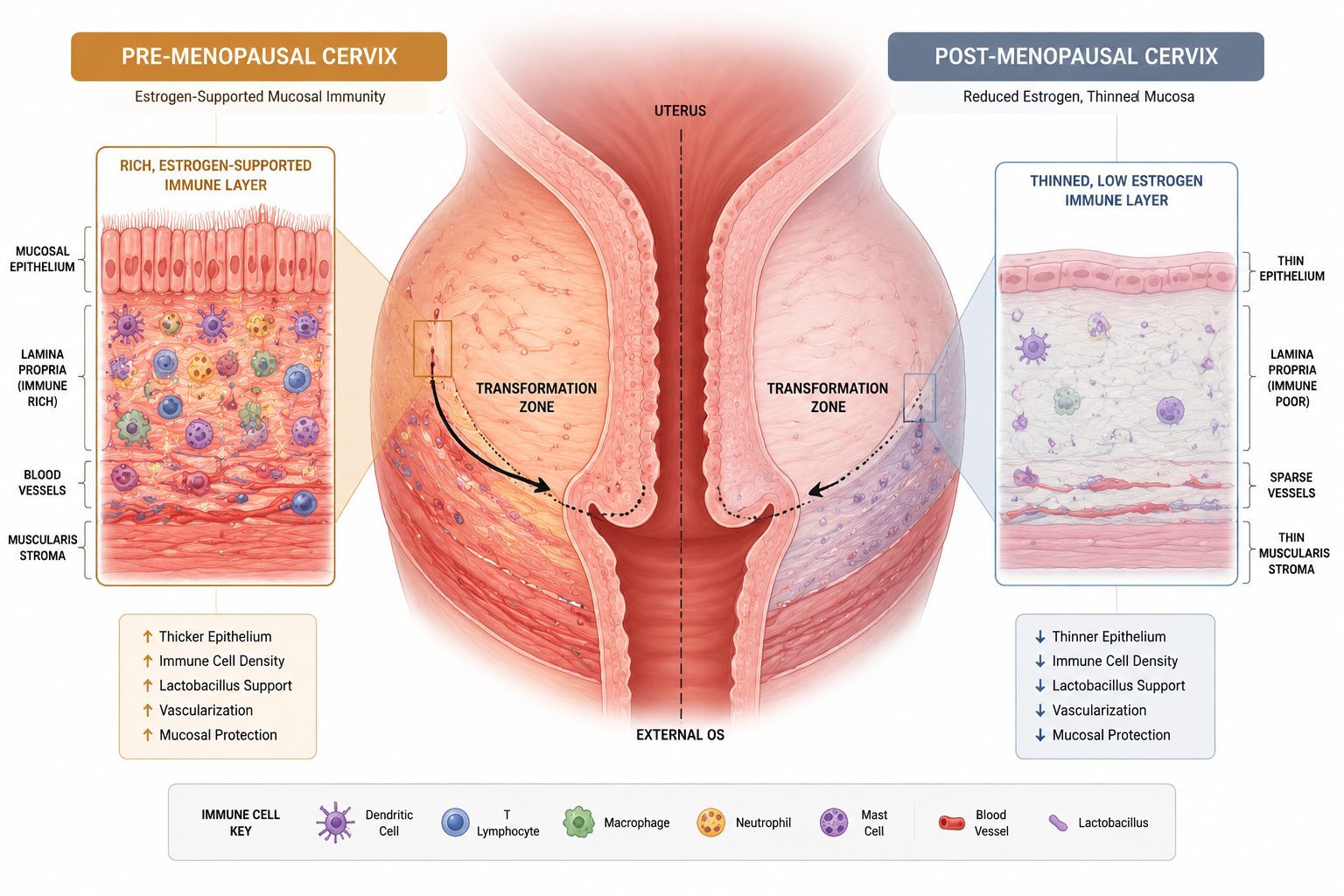
Estrogen does more than regulate the reproductive cycle. It actively supports the mucosal immune environment of the cervix. The cervical epithelium — the tissue layer where HPV establishes infection — is estrogen-responsive. Estrogen promotes the production of secretory immunoglobulins and supports the local immune cell populations that surveil cervical tissue for abnormal cells.
When estrogen levels drop sharply during and after menopause, this local immune support diminishes. The cervical epithelium becomes thinner and more atrophic. The mucosal immune layer weakens. The result is a local environment that is less equipped to mount an effective immune response against HPV-infected cells — even if the systemic immune system is functioning reasonably well.
There is a second anatomical change worth understanding. Before menopause, the transformation zone — the area of the cervix most vulnerable to HPV-related cell changes — is typically visible and accessible during a standard Pap smear. After menopause, the transformation zone shifts inward as the cervix atrophies, making it less accessible and, in some cases, making cell changes harder to detect. The NCI's guidance on HPV and cervical cancer addresses this anatomical context in its post-menopausal screening recommendations.
It is important to frame this accurately: the mechanistic link between estrogen decline and HPV persistence is biologically plausible and supported by observational research, but it is not yet definitively established in controlled trials. What is established is that post-menopausal women face a more challenging immune environment for HPV clearance — and that this reality deserves to be named directly rather than glossed over.
Why "Watch and Wait" Lands Differently at 50
"Watch and wait" is not wrong advice. It is medically appropriate, and monitoring is genuinely important. But the phrase carries an implicit assumption: that the immune system will eventually do its job, and that time is on your side.
At 27, time largely is on your side. The CDC's HPV data confirms that most HPV infections in younger adults clear within one to two years. The biological tailwind is real. Watching and waiting makes sense because the immune system is actively working in the background, and the odds favor clearance.
At 52, the tailwind is weaker. The immune system is still working — but at a lower baseline, with reduced NK cell activity and slower T-cell response. Waiting passively for clearance that may not come at the same pace is a different proposition. It is not wrong to monitor. It is insufficient to monitor and do nothing else.
This is not an argument against medical oversight — it is an argument for pairing consistent monitoring with active immune support. The women who navigate HPV after 50 most successfully tend to be those who treat it as a condition requiring active management rather than passive observation. That means addressing every modifiable factor that affects immune function: sleep, stress, nutrition, vitamin D status, and targeted supplementation where the evidence supports it.
For a broader look at the factors that determine whether HPV clears or persists, the article on why some people clear HPV faster than others covers the full picture — including the immune factors that are most relevant to this age group.
How Screening Changes After Menopause
One of the least-discussed complications of HPV after 50 is how menopause affects the accuracy and interpretation of cervical screening itself.
Atrophic changes can complicate Pap results. Estrogen deficiency causes the cervical and vaginal epithelium to thin and become atrophic. These atrophic changes can produce cellular appearances on a Pap smear that are difficult to distinguish from low-grade dysplasia. The result can be an abnormal Pap result that reflects hormonal change rather than HPV-related cell changes — or, conversely, true cell changes that are harder to identify against an atrophic background.
Some providers recommend a short course of topical vaginal estrogen before a Pap smear in post-menopausal women to restore the epithelium temporarily and improve test accuracy. This is a clinical decision that should be made with your provider — but it is worth asking about if you have received an inconclusive or difficult-to-interpret result.
HPV co-testing remains reliable after menopause. While Pap smear interpretation can be complicated by atrophic changes, the HPV DNA test itself is not affected by hormonal status. Co-testing — a Pap smear combined with an HPV test — remains the most informative screening approach for post-menopausal women with known persistent infection.
The "stop screening at 65" guidance does not apply universally. Many women are told that cervical screening can be discontinued after age 65. This guidance applies specifically to women with a consistently negative screening history over the preceding decade. Women with known persistent HPV — regardless of age — should continue monitoring. Stopping screening because of age alone, in the context of a known active infection, is not appropriate. Monitoring frequency and approach should be determined by your provider based on HPV strain, cytology results, and individual history.
| Situation | Recommended Approach |
|---|---|
| HPV positive, normal Pap | Co-test in 12 months |
| High-risk HPV (16 or 18) | Colposcopy referral typically indicated |
| CIN 1 | Monitor per provider guidance; frequency varies |
| CIN 2 or CIN 3 | Treatment discussion with provider — do not defer |
| Post-menopausal, any persistent HPV | Continue monitoring; do not self-discharge from screening |
What You Can Actually Do
The biological challenges of HPV after 50 are real. They are not fixed.
Immune function — even aging immune function — responds to deliberate support. The immune system at 52 is not the immune system at 28, but it is still capable of mounting an effective response to HPV when given the conditions to do so. The following sections cover the specific interventions with the strongest evidence base for this age group: targeted supplementation, vitamin D optimization, sleep quality, and stress regulation. None of these is a cure. Together, they represent the most evidence-informed approach available to women managing HPV after 50.
AHCC and Immune Support After 50
Among the supplements that have been studied in the context of HPV clearance, AHCC (Active Hexose Correlated Compound) stands apart for one specific reason: it is the only supplement with a published, placebo-controlled human clinical trial targeting HPV clearance.
The trial was led by Dr. Judith Smith at the University of Texas Health Science Center at Houston. It enrolled women with persistent high-risk HPV infections — a profile that by definition includes older women, since persistence is more common with age. The published research from Dr. Smith's team found that a meaningful proportion of participants in the AHCC arm achieved HPV clearance, compared to the placebo group. The results were published in peer-reviewed literature and are accessible through PubMed.
It is important to frame this accurately. AHCC is not an approved treatment for HPV. The trial results are promising and preliminary — they support further investigation and warrant serious consideration as part of a broader immune support protocol, but they do not constitute proof of efficacy in a clinical treatment sense. Research suggests AHCC may support NK cell activity and immune modulation — these mechanisms are proposed and research-supported, not definitively established.
The protocol used in clinical research: 3 grams per day, taken on an empty stomach, for a minimum of six months. For women over 50 facing additional immune challenges from senescence and hormonal change, some practitioners extend this protocol to nine months — but this reflects clinical practice rather than a published protocol, and individual decisions should be made with a healthcare provider.
For a thorough review of the clinical evidence, the article does AHCC really help clear HPV covers the trial design, results, and limitations in detail. For guidance on dosing, the article on what dosage of AHCC to take for HPV addresses the clinical protocol and practical considerations.
NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility. At 3 grams per day, the clinical protocol requires approximately four to five capsules daily, taken on an empty stomach — ideally in the morning, at least 30 minutes before eating.

Vitamin D — The Most Common Deficiency
Vitamin D deficiency is more prevalent after 50 than at any other adult life stage, for reasons that are compounded and often overlooked.
Skin synthesis of vitamin D from sunlight becomes less efficient with age. Older adults typically spend less time outdoors. And the conversion of vitamin D to its active hormonal form — calcitriol — becomes less efficient as kidney function gradually declines with age. The result is that many women over 50 are vitamin D deficient even if they believe their diet and sun exposure are adequate.
This matters directly for HPV clearance. Vitamin D receptors are present on nearly every immune cell. Both T-cells and NK cells require adequate vitamin D to function at full capacity. Deficiency is associated with impaired immune surveillance — the exact mechanism that is already under pressure from immune senescence. According to the NIH Office of Dietary Supplements, vitamin D plays a well-established role in modulating both innate and adaptive immune function.
The practical recommendation is straightforward: test your 25(OH)D blood level. A level below 20 ng/mL is classified as deficient; below 30 ng/mL is considered insufficient. For immune function specifically, many practitioners target a range of 40 to 60 ng/mL — though optimal targets should be discussed with your provider. Supplementation based on a confirmed deficiency is evidence-based, widely recommended, and inexpensive. It is one of the highest-value interventions available for immune support after 50.
Sleep and Stress at 50
Sleep and stress are rarely discussed in clinical HPV conversations, but both have direct, measurable effects on immune function — and both are significantly harder to manage after 50.
Sleep disruption is common and immunologically costly. Post-menopausal women experience higher rates of sleep disruption than any other demographic: night sweats, hormonal fluctuation, anxiety, and the physiological changes of menopause itself all interfere with sleep architecture. The immune consequences are not trivial. Cytokine production, NK cell activity, and T-cell function are all regulated in part during sleep. Consistently poor sleep — fewer than seven hours, or fragmented sleep — suppresses immune function in ways that directly overlap with immune senescence. The two compound each other.
The target is seven to nine hours of consistent, quality sleep. This is not a platitude — it is a clinically supported immune intervention. Achieving it after 50 may require addressing the underlying causes of disruption: discussing hormonal management with a provider, optimizing sleep environment, and in some cases working with a sleep specialist. The effort is worth it from an immune function standpoint.
Chronic stress is different from acute stress — and more damaging. Women in their 50s often carry sustained stress loads: aging parents requiring care, career transitions, relationship changes, and the psychological weight of managing a health condition like HPV in relative isolation. Chronic elevated cortisol suppresses both NK cell activity and T-cell function. This is not stress as a vague wellness concept — it is a measurable immunological effect.
Evidence-based approaches to stress regulation include Mindfulness-Based Stress Reduction (MBSR), regular moderate exercise (which has independent immune benefits), and consistent social connection. These are harder to achieve in this life stage than they are to recommend — acknowledging that reality is part of taking it seriously. Small, consistent changes in any of these areas have cumulative immune benefit over the months-long timeframe relevant to HPV clearance.
Monitoring — What to Expect
Consistent monitoring is not optional for women over 50 with persistent HPV. It is the clinical foundation on which everything else rests. The goal of immune support is to facilitate clearance — but monitoring is what ensures that any progression toward cell changes is caught and addressed early.
The risk context matters here. Understanding how HPV relates to cancer risk is important for calibrating the urgency of monitoring — particularly for women carrying high-risk strains. Not all HPV strains carry equal risk, and what HPV 16 and HPV 18 mean specifically is worth understanding if you have received a strain-specific result.
| Situation | Recommended Monitoring Approach |
|---|---|
| HPV positive, normal Pap | Co-test in 12 months |
| High-risk HPV (16 or 18) | Colposcopy referral typically indicated |
| CIN 1 | Monitor per provider guidance; do not defer |
| CIN 2 or CIN 3 | Treatment discussion — prompt, not passive |
| Post-menopausal, any persistent HPV | Continue monitoring regardless of age |
Several points deserve emphasis for women over 50 specifically:
- Colposcopy should not be deferred because of age. Some women over 50 are implicitly or explicitly discouraged from colposcopy on the grounds that treatment is more complex post-menopause. This reasoning does not justify deferring diagnostic evaluation.
- Post-menopausal atrophy may require estrogen preparation before Pap. Discuss this with your provider if you have had inconclusive results.
- The "stop at 65" screening guideline does not apply to women with known persistent infection. If you have active HPV, age alone is not a reason to stop monitoring.
- Monitoring frequency should be provider-determined based on your specific HPV strain, cytology findings, and personal history — not based on general population guidelines that were not designed for your situation.

Frequently Asked Questions
Is HPV common in women over 50?
HPV is more common in women over 50 than most people realize. While prevalence peaks in younger adults, a second prevalence peak has been observed in women over 45 to 50 in several population studies. This second peak is thought to reflect both new exposures and the reactivation of latent infections that the immune system had previously suppressed. Women over 50 are not past the age of HPV risk — they are in a phase where the immune system is less equipped to manage it.
Can HPV clear on its own after 50?
Yes — but the process is slower and less reliable than at younger ages. Immune senescence reduces the efficiency of viral clearance, and the hormonal changes of menopause affect local cervical immunity. Clearance is still possible and does occur in women over 50, but it is less likely to happen within the 12 to 24 month window that applies to younger women. Active immune support — rather than passive waiting — is a more appropriate strategy for this age group.
Should I get the HPV vaccine if I am over 50?
The HPV vaccine (Gardasil 9) is FDA-approved for adults up to age 45. It is not currently approved for routine use in adults over 45, and it does not treat an existing HPV infection — it prevents new infections from the strains it covers. For women over 50 with an existing diagnosis, the vaccine is unlikely to be recommended by most providers, though individual circumstances vary. This is a conversation to have with your healthcare provider based on your specific strain, history, and exposure context.
Does menopause make HPV more dangerous?
Menopause does not change the inherent risk profile of a given HPV strain, but it does create conditions that may allow an existing infection to persist longer and cell changes to develop more readily. The reduction in estrogen-supported mucosal immunity, combined with immune senescence, means that the body's natural defenses against HPV-related cell changes are operating at a lower level. This makes consistent monitoring more important after menopause, not less.
How long does it typically take to clear HPV after 50?
There is no reliable average for women over 50 because the published clearance data is heavily weighted toward younger populations. What the available evidence suggests is that clearance timelines are longer and less predictable after 50. Women in clinical AHCC research — which enrolled women with persistent high-risk HPV — saw results over a six-month minimum protocol. For women over 50 with additional immune challenges, some practitioners extend immune support protocols to nine months or longer. Individual timelines depend on HPV strain, immune status, lifestyle factors, and whether active immune support is being pursued.
Conclusion
HPV after 50 is a harder biological situation than most HPV content acknowledges. Immune senescence is real. The hormonal changes of menopause affect local cervical immunity in ways that matter. And the standard reassurance — that the immune system will clear the virus in time — carries less weight when the immune system is operating at a reduced baseline.
None of this is reason for fatalism. It is reason for a more deliberate approach.
The women who navigate HPV after 50 most successfully are those who combine consistent medical monitoring with active immune support — who treat this as a condition requiring engagement rather than passive observation. That means working with a provider who takes post-menopausal HPV seriously, maintaining a monitoring schedule appropriate to their specific situation, and addressing every modifiable factor that affects immune function.
Concrete next steps:
- Confirm your HPV strain with your provider if you have not already. High-risk strains (particularly 16 and 18) require a different monitoring approach than lower-risk strains.
- Test your vitamin D level (25(OH)D blood test). Address any deficiency with supplementation under provider guidance before expecting optimal immune function.
- Review your monitoring schedule with your provider. If you have been told to "just wait and see" without a clear follow-up plan, ask for specifics: co-test at what interval, colposcopy if what threshold, and what the criteria are for escalation.
- Evaluate AHCC as part of your immune support protocol. Review the clinical evidence, discuss it with your provider, and if you proceed, commit to the full six-month minimum protocol at the clinically studied dose.
- Prioritize sleep and stress management as immune interventions, not lifestyle luxuries. If post-menopausal sleep disruption is affecting your sleep quality, address it directly — it has measurable immune consequences.
Related Reading
- The biological and immune factors behind why HPV fails to clear in some people — a detailed look at persistence mechanisms.
- A comprehensive review of the clinical evidence for AHCC and HPV clearance, including trial design and results.
- Practical guidance on steps to take after an HPV diagnosis — an evidence-based action plan.
- What the research shows about AHCC for general immune resilience and healthy aging — relevant context for women over 50 thinking about long-term immune health.
References
- CDC — HPV fact sheet
- NCI — HPV and cervical cancer
- NIH — Vitamin D fact sheet (Office of Dietary Supplements)
- NIH / PubMed — Immunosenescence and aging immune function (PMC3582124)
- WHO — HPV and cervical cancer fact sheet
- PubMed — AHCC clinical research database
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







