


Roughly 90% of HPV infections clear on their own within two years — without treatment, without intervention, and without ever progressing toward cancer. If a diagnosis has left you searching for answers about HPV and cancer risk, the most important thing to understand first is this: a positive HPV result is not a cancer diagnosis, and for the vast majority of people, it never will be. What this article addresses is the more precise and more useful question: given that HPV is present, what actually determines whether it becomes dangerous — and which of those factors can be changed?
Key Takeaways
- Approximately 90% of HPV infections clear naturally within two years without causing cancer or lasting harm.
- HPV is responsible for roughly 5% of all cancers worldwide — meaning the overwhelming majority of infections do not progress.
- Cancer requires a specific, rare sequence of events: persistent infection with a high-risk strain, over many years, in the absence of detection and intervention.
- Several of the most important risk factors — including smoking, vitamin D status, and screening adherence — are fully or partially within your control.
- Clearing HPV removes the biological precondition for HPV-related cancer; supporting immune clearance is therefore a meaningful risk-reduction strategy.
In This Article
- Most HPV never becomes cancer
- What actually determines cancer risk
- HPV strain — the single biggest factor
- Persistence — why time matters
- Modifiable risk factors you can act on
- Why screening is the most powerful intervention
- The HPV vaccine and cancer prevention
- Clearing HPV — removing the precondition
- Frequently asked questions
Most HPV Never Becomes Cancer
A positive HPV test result is far more common than most people realize — and far less dangerous than most people fear. According to the CDC, approximately 90% of HPV infections clear on their own within two years, driven by a healthy immune response. The body recognizes and suppresses the virus without any medical treatment in the vast majority of cases.
HPV is the most common sexually transmitted infection globally. The World Health Organization estimates that HPV is responsible for approximately 5% of all cancers worldwide. That figure is significant — it represents hundreds of thousands of lives affected each year — but it also means that the overwhelming majority of the estimated 300 million people living with HPV at any given time will never develop cancer from it.
Cancer does not follow automatically from HPV infection. It requires a specific, rare sequence of events: infection with a high-risk strain, failure of the immune system to clear that strain, persistence of the virus over many years, accumulation of cellular damage, and the absence of screening that would otherwise catch precancerous changes before they progress. Every one of those steps represents an opportunity for the process to be interrupted.
"A positive HPV result is not a cancer diagnosis. For most people, it is a temporary infection that the immune system will resolve."
Understanding this is not about minimizing a real risk. It is about responding to the actual risk accurately — which is the only way to take effective action.
What Actually Determines HPV and Cancer Risk
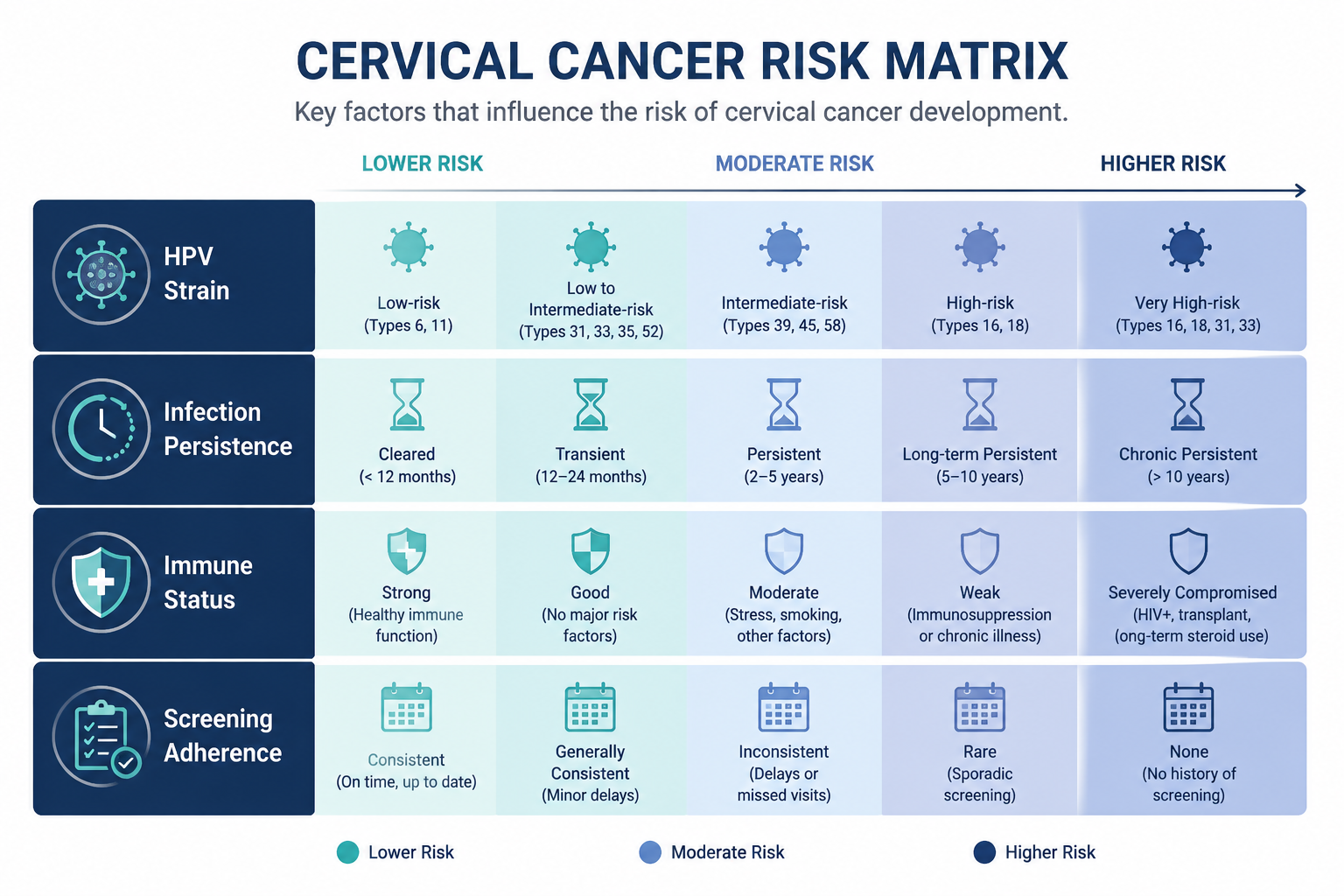
HPV and cancer risk is not a binary outcome — it is a product of multiple interacting factors, most of which exist on a spectrum. Understanding these factors allows for a rational, prioritized response rather than generalized anxiety.
The table below summarizes the primary determinants:
| Risk Factor | Impact on Cancer Risk | Modifiable? |
|---|---|---|
| HPV strain (high vs. low risk) | Highest | No — but clearance is |
| Infection persistence | Very high | Partially — immune support |
| Immune status | High | Partially — lifestyle factors |
| Screening adherence | High | Yes — fully in your control |
| Smoking | Moderate-high | Yes |
| HIV or immunosuppression | High | Partially — management matters |
| Vitamin D deficiency | Moderate | Yes |
| Co-infections (chlamydia, herpes) | Moderate | Yes |
| Time since infection | High | N/A — underscores screening importance |
This is a risk matrix, not a checklist of doom. Each factor is something to understand and address — not a predetermined outcome. The sections that follow examine the most important of these factors in detail.
HPV Strain — The Single Biggest Factor
Not all HPV strains carry the same cancer risk. Of the more than 200 known HPV types, approximately 14 are classified as high-risk — meaning they have the biological capacity to cause cancer if they persist long enough. Low-risk strains, such as HPV 6 and 11, cause genital warts but are not associated with cancer.
The National Cancer Institute identifies HPV 16 and HPV 18 as the strains responsible for the majority of HPV-related cancers — together accounting for approximately 70% of cervical cancers. Other high-risk strains, including HPV 31, 33, 45, 52, and 58, account for a significant portion of the remainder.
Knowing which strain is present matters clinically because it informs monitoring frequency. A diagnosis with HPV 16 or 18 typically warrants more immediate follow-up, such as colposcopy referral, compared to other high-risk strains. For a detailed breakdown of what these specific strains mean for your health, see why HPV 16 and HPV 18 are the most dangerous HPV strains.
It is worth emphasizing: even HPV 16 and 18 clear naturally in the majority of cases. The strain distinction matters for monitoring urgency — not for immediate alarm. The mechanism by which high-risk strains drive cancer development involves specific viral proteins; for a full explanation of that biology, see how does HPV cause cancer.
HPV does not only affect the cervix. High-risk strains are also associated with oropharyngeal, anal, penile, vulvar, and vaginal cancers. The rise in HPV-related throat and mouth cancers is a growing area of clinical concern — a topic covered in depth in oral HPV: the silent infection no one talks about.
Persistence — Why Time Matters
If there is a single concept that reframes HPV and cancer risk most usefully, it is this: it is not HPV infection that causes cancer — it is persistent infection with a high-risk strain that goes undetected and untreated over many years.
The typical timeline from initial HPV infection to invasive cervical cancer is 10 to 20 years. That is not a reason for complacency — it is a reason for structured, consistent monitoring. Every year that HPV is detected and tracked is a year during which the progression can be interrupted. Precancerous changes (cervical intraepithelial neoplasia, or CIN) develop well before cancer does, and they are highly treatable when caught.
Persistence itself is not inevitable. The immune system clears most infections within two years. When it does not, the reasons are often identifiable and addressable — including immune suppression, smoking, nutritional deficiencies, and high viral load. For a comprehensive look at why some infections persist when others do not, see why HPV doesn't clear in some people.
The practical implication is straightforward: the goal is not to wait and hope, but to actively support clearance while maintaining consistent screening. Both strategies work in parallel.
Modifiable Risk Factors You Can Act On

This section is where HPV and cancer risk becomes genuinely actionable. Several of the factors that most influence whether HPV persists and progresses are within your direct control.
Smoking
Smoking is the single largest modifiable co-factor for HPV persistence and cervical cancer progression. Tobacco compounds directly damage cervical epithelial cells and impair local immune surveillance — the immune activity that normally suppresses HPV at the site of infection. Multiple large studies have found that smokers have significantly higher rates of persistent HPV infection and cervical cancer compared to non-smokers. For anyone with a current HPV diagnosis who smokes, cessation is the highest-impact action available.
HIV and Immunosuppression
People living with HIV have up to five times higher rates of cervical cancer compared to the general population, according to WHO data. Other forms of immunosuppression — including organ transplant medications and long-term corticosteroid use — also significantly increase HPV persistence and cancer risk. If immunocompromised, discuss enhanced monitoring intervals with your healthcare provider. This is not optional.
Vitamin D Deficiency
Vitamin D is essential for normal immune function, including the T-cell and natural killer cell activity that suppresses viral infections. Research published through the NIH Office of Dietary Supplements documents the broad role of vitamin D in immune regulation. Studies have associated vitamin D deficiency with impaired HPV clearance and higher rates of HPV persistence. Testing vitamin D levels and correcting deficiency — through supplementation and appropriate sun exposure — is a low-cost, low-risk intervention with meaningful potential benefit.
Long-Term Oral Contraceptive Use
Some studies associate prolonged oral contraceptive use — typically defined as five or more years — with a modestly increased cervical cancer risk in HPV-positive women. The mechanism is not fully established, and the absolute risk increase is small. This does not mean discontinuing contraception without medical guidance, but it is worth discussing with your provider if it applies to your situation.
Co-Infections
Evidence from several studies suggests that co-infection with certain sexually transmitted infections — including chlamydia and herpes simplex virus type 2 — may increase cervical cancer risk in HPV-positive women. The proposed mechanisms include local inflammation and immune modulation. Routine STI screening is appropriate for anyone with a current HPV diagnosis.
Why Screening Is the Most Powerful Intervention

Cervical cancer is one of the most preventable cancers in existence — not because it is rare, but because the window between HPV infection and invasive cancer is long, measurable, and highly interruptible. Pap smears detect cellular changes (CIN) years before cancer develops. HPV co-testing identifies the presence of high-risk strains. Together, these two tools allow clinicians to intervene at the precancerous stage — which is highly treatable with straightforward procedures.
Missing screening is the highest-risk decision someone with HPV can make. It does not reduce anxiety; it removes the opportunity to catch a problem early.
The table below provides general screening guidance. Individual schedules are determined by your provider based on your specific results and history — always follow their recommendations over general guidelines.
| Situation | General Guideline |
|---|---|
| Age 21–29, no HPV detected | Pap smear every 3 years |
| Age 30–65, no HPV detected | Co-test every 5 years or Pap every 3 years |
| HPV positive, normal Pap | Co-test in 1 year |
| High-risk HPV (16 or 18) | Colposcopy referral typically recommended |
| Any abnormal Pap result | Follow-up per provider guidance |
Note: guidelines vary by country, clinical body, and individual history. The American College of Obstetricians and Gynecologists and the U.S. Preventive Services Task Force publish updated recommendations periodically. Your provider will tailor your schedule accordingly.
The HPV Vaccine and Cancer Prevention
Gardasil 9 is the most effective cancer prevention tool currently available for HPV-related disease. It protects against nine HPV strains — including HPV 16, 18, 31, 33, 45, 52, and 58 — which together account for the majority of HPV-related cancers globally. The vaccine prevents new infection with these strains; it does not treat an existing infection.
Vaccination is routinely recommended through age 26. For adults aged 27 to 45, the CDC recommends shared decision-making with a healthcare provider — the benefit depends on prior HPV exposure and individual risk factors. Even people who have already tested positive for one HPV strain may benefit from vaccination, as it provides protection against strains not yet encountered.
If unvaccinated, discussing the vaccine with your provider is worthwhile regardless of current HPV status or age. It remains one of the clearest examples of a genuinely cancer-preventive intervention available in clinical practice.
Clearing HPV — Removing the Precondition

The relationship between immune clearance and HPV and cancer risk is direct: HPV cannot cause cancer if it is no longer present. Clearing the virus removes the biological precondition for HPV-related cancer. This makes supporting immune clearance a meaningful strategy — not just for a negative test result, but for genuine risk reduction.
The foundational immune support measures are well-established: smoking cessation (the highest-impact single action), correcting vitamin D deficiency, prioritizing consistent sleep, managing chronic stress, and maintaining a diet that supports immune function. These are not peripheral lifestyle suggestions — they directly influence the immune activity responsible for HPV suppression.
Beyond these foundations, one supplement has attracted meaningful clinical attention. AHCC (Active Hexose Correlated Compound) is a proprietary extract derived from shiitake mushroom mycelia. It is the only supplement with a published, placebo-controlled human clinical trial specifically targeting HPV clearance. That research, conducted by Dr. Judith Smith at the University of Texas Health Science Center at Houston and published in peer-reviewed literature accessible via PubMed, demonstrated promising results in a small but rigorously designed trial. The research-validated protocol used in that study was 3 grams per day taken on an empty stomach for a minimum of six months.
It is essential to frame this accurately. AHCC does not prevent cancer directly, and no claim that it "reduces cancer risk" as an established fact should be made. What the preliminary evidence suggests is that AHCC may support immune clearance of HPV — and clearing HPV removes the precondition for HPV-related cancer. That is the honest, clinically grounded framing.
NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility. At the research-validated dose of 3 grams per day, this requires approximately four to five capsules daily, taken fasted.
For a detailed look at the mechanism by which AHCC may support HPV clearance, see how does AHCC clear HPV. For a review of the clinical trial evidence, see does AHCC really help clear HPV.
Frequently Asked Questions
Does having HPV mean I will get cancer?
No. A positive HPV result is not a cancer diagnosis and, for most people, will never become one. Approximately 90% of HPV infections clear naturally within two years. Cancer requires persistent infection with a high-risk strain over many years, in the absence of detection and treatment. The vast majority of people with HPV will not develop cancer from it, particularly those who maintain consistent screening and address modifiable risk factors.
Which HPV strains are most likely to cause cancer?
HPV 16 and HPV 18 carry the highest cancer risk and together account for approximately 70% of cervical cancers. Other high-risk strains — including HPV 31, 33, 45, 52, and 58 — account for a significant portion of the remainder. Low-risk strains such as HPV 6 and 11 cause genital warts but are not associated with cancer. Knowing your strain type helps your provider determine appropriate monitoring frequency.
How long does it take for HPV to develop into cancer?
The typical timeline from initial HPV infection to invasive cancer is 10 to 20 years. This is not a reason for complacency — it is the reason that consistent screening is so effective. Precancerous changes develop well before cancer does and are highly treatable when detected. Every screening appointment is an opportunity to interrupt the progression.
Does clearing HPV reduce my cancer risk?
Yes, in a direct and meaningful way. HPV cannot cause cancer if it is no longer present. Clearing the virus removes the biological precondition for HPV-related cancer. This is why supporting immune clearance — through lifestyle measures, consistent screening, and potentially evidence-based supplements — is a legitimate and worthwhile risk-reduction strategy.
What is the single most important thing I can do to reduce my HPV-related cancer risk?
For most people, the answer is consistent screening. Missing Pap smears and HPV co-testing removes the opportunity to catch precancerous changes before they progress — and that window is long and reliable. For people who smoke, cessation is the highest-impact single action available. For everyone, addressing vitamin D deficiency, maintaining a healthy immune system, and staying current with vaccination recommendations all contribute meaningfully to reducing HPV and cancer risk.
Conclusion
HPV and cancer risk is a subject that deserves accurate information, not generalized fear. The evidence is clear: most HPV infections resolve on their own, cancer requires a specific and interruptible sequence of events, and several of the most important risk factors are within your control.
Actionable next steps:
- Confirm your HPV strain type with your healthcare provider if not already known — this determines appropriate monitoring frequency and urgency.
- Schedule and maintain regular screening — Pap smears and HPV co-testing are the most powerful tools available for preventing HPV-related cancer. Do not skip or delay appointments.
- Address modifiable risk factors — if you smoke, prioritize cessation above all other interventions. Check your vitamin D level and correct any deficiency. Manage stress and sleep consistently.
- Discuss vaccination with your provider if unvaccinated — Gardasil 9 protects against the strains responsible for the majority of HPV-related cancers and may still benefit you even with an existing diagnosis.
- Support immune clearance actively — consider evidence-based options such as AHCC alongside lifestyle measures, and discuss with your provider whether the research-validated protocol is appropriate for your situation.
Related Reading
- For a complete breakdown of how HPV progresses to cancer at the cellular level, see how does HPV cause cancer.
- To understand what makes certain strains significantly more dangerous, read why HPV 16 and HPV 18 are the most dangerous HPV strains.
- For accounts of people who have navigated HPV clearance with AHCC, visit AHCC HPV success stories.
- For a practical guide on what to do immediately after a positive diagnosis, see I have HPV — now what? 8 steps to clear the virus naturally.
References
- CDC — HPV fact sheet: https://www.cdc.gov/hpv
- WHO — HPV and cervical cancer (2023): https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer
- NCI — HPV and cancer: https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
- NIH Office of Dietary Supplements — Vitamin D and immune function: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- PubMed — AHCC clinical research (Smith JA et al.): https://pubmed.ncbi.nlm.nih.gov/
- PMC11850150 — HPV-associated cancer complexity review (2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC11850150/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







