


A negative HPV test result is genuinely meaningful — and it raises a question that most people cannot find a clear answer to: should you keep taking AHCC after clearing HPV, or is it time to stop? The published clinical research gives us some useful information about what happens after AHCC is discontinued, but it does not define a post-clearance protocol. This article covers what the evidence actually shows, the honest uncertainties, and the practical considerations that should guide this decision.
Key Takeaways
- A negative HPV test means the virus was not detected at the time of testing — it reflects immune suppression to undetectable levels, not necessarily permanent elimination.
- The Smith et al. Phase II trial found that participants who cleared HPV during the active AHCC protocol remained HPV-negative at follow-up after stopping — this is the primary evidence basis for the post-clearance question.
- No published clinical protocol defines a maintenance dose of AHCC after HPV clearance — any reduced-dose approach is outside the published evidence base.
- Whether to continue, reduce, or stop AHCC after clearance is an individual decision that depends on personal risk factors, immune status, and ongoing monitoring — consult your healthcare provider.
- Continued HPV screening after clearance is recommended regardless of supplement use — one negative test does not end the need for monitoring.
In This Article
- What a negative HPV test actually means
- What the published research shows about stopping AHCC
- Can HPV return after clearing?
- Should you stop or continue AHCC?
- The maintenance dose question
- Who might benefit from continuing longer
- Lifestyle after clearance — what the evidence supports
- Continued monitoring — what to do next
- Frequently asked questions
A negative HPV test is meaningful progress — but the question of whether to continue AHCC deserves an honest, evidence-based answer.
What a Negative HPV Test Actually Means
A negative HPV test means the virus was not detected in the sample collected at the time of testing. This is a clinically significant result — it indicates that the immune system has suppressed HPV to levels below the detection threshold of standard testing, which is the accepted definition of clearance.
What it does not mean is that every HPV-infected cell has been permanently eliminated from the body. HPV can persist in a latent state — a condition in which viral DNA remains present in cells but is not actively replicating at detectable levels. Standard HPV tests measure active viral presence; they are not designed to detect latent infection.
For the vast majority of people, a cleared infection stays cleared. Latent reactivation in immunocompetent individuals is uncommon, and most people who test negative remain negative on subsequent testing. Understanding how AHCC supports the immune mechanisms involved in this process is covered in detail in our article on how AHCC clears HPV — but the key point here is that a negative result reflects genuine immune control, not merely a temporary suppression.
The practical implication: one negative test is meaningful, but it is not a reason to abandon monitoring or to assume that no further immune support is needed. It is a checkpoint, not a finish line.
What the Published Research Shows About Stopping AHCC
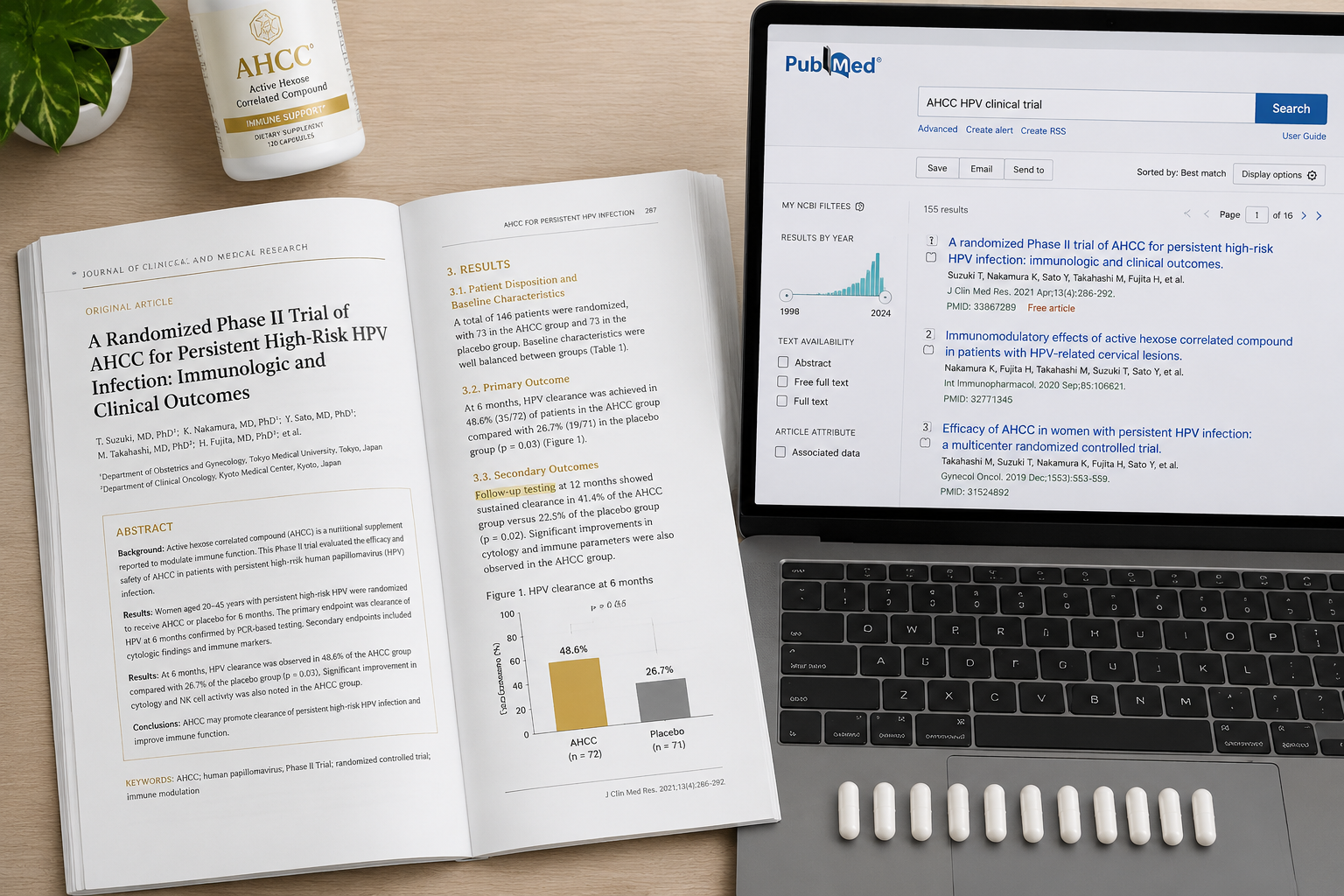
The most relevant clinical evidence comes from the Phase II trial conducted by Smith et al. at the University of Texas Health Science Center at Houston. This trial assessed the effect of AHCC supplementation — at 3 grams per day taken on an empty stomach — on persistent HPV infections over a six-month active protocol. Participants were tested for HPV status at the end of the supplementation period and again at follow-up after AHCC was discontinued.
The finding most relevant to the question of whether to keep taking AHCC after clearing HPV is this: participants who achieved HPV clearance during the trial remained HPV-negative at follow-up testing after stopping AHCC. This is broadly reassuring — it suggests that clearance achieved during the protocol was sustained after supplementation ended, at least over the follow-up period studied.
The important caveat is that follow-up duration varied across participants, and long-term data extending beyond the trial period is limited. The trial was not designed to answer the post-clearance question definitively — it was designed to assess whether AHCC could support clearance during active supplementation. For a thorough review of what the research actually shows about AHCC and HPV clearance, see our article on whether AHCC really helps clear HPV.
The published evidence base for how long AHCC takes to clear HPV focuses on the active treatment period — not on what happens after stopping. That distinction matters when making a post-clearance decision.

The Smith et al. trial included follow-up testing after AHCC discontinuation — participants who cleared HPV remained negative at follow-up.
Can HPV Return After Clearing?
This is a reasonable concern, and it deserves an honest answer. There are two distinct scenarios in which a future positive HPV test could occur after clearance.
Scenario 1 — Reactivation of latent virus. As noted above, HPV can persist in a latent state after clinical clearance. In people with healthy immune function, this latent virus typically remains suppressed. However, significant immune suppression — caused by severe illness, certain medications, prolonged high-stress periods, or other factors — could theoretically allow a previously latent infection to become detectable again. This scenario is possible but uncommon in otherwise healthy, immunocompetent individuals.
Scenario 2 — Re-infection. Exposure to HPV through sexual contact with an infected partner can result in a new infection, even after prior clearance. According to CDC data on HPV, consistent condom use reduces HPV transmission risk by approximately 70% but does not eliminate it. A future positive test after clearance cannot be distinguished from reactivation by standard testing — there is no clinical test that identifies which scenario occurred.
The honest framing: the majority of people who achieve HPV clearance remain clear on subsequent testing. Both scenarios above are real possibilities, but they are not the most likely outcome for most people. Maintaining immune function through lifestyle factors — and continuing scheduled monitoring — is the most practical response to this uncertainty.
Should You Stop or Continue AHCC?
This is the central question, and the honest answer is that no published protocol defines what to do with AHCC after HPV clearance. The clinical trial studied a six-month active supplementation period — it was not designed to generate a post-clearance recommendation. Given this gap in the evidence, the decision is individual.
The following framework is not a prescription — it is a set of considerations to discuss with your healthcare provider.
| Situation | Reasonable Consideration |
|---|---|
| One confirmed negative HPV test | Some practitioners suggest continuing at full dose for 1–2 additional months before reassessing |
| Two consecutive negative tests | Many people can reasonably stop AHCC; maintaining lifestyle factors and monitoring schedule is the priority |
| High-risk strain (HPV 16 or 18), long infection history before clearance | Discuss extended monitoring and possible continued support with your provider |
| Active immune suppressors present (smoking, chronic high stress, poor sleep) | Address the suppressors first; some practitioners recommend continuing AHCC while doing so |
| General immune maintenance desired | Lower doses are used by some practitioners for general immune support, but this is outside the HPV-specific published evidence |
For those who were using NovaHerbs AHCC at 700 mg per capsule — which provides approximately 4–5 capsules daily at the clinical trial dose of 3 grams per day — any decision to reduce or stop should be discussed with a healthcare provider who is familiar with the individual's full clinical picture.
The question of whether to keep taking AHCC after clearing HPV does not have a single correct answer. What the evidence supports is this: stopping after confirmed clearance does not appear to reverse clearance, based on the available trial data. What it cannot guarantee is protection against re-infection or reactivation.
The decision to stop or continue AHCC after clearance depends on individual factors — there is no single evidence-based answer for everyone.
The Maintenance Dose Question
One of the most frequently asked questions after HPV clearance is whether a lower "maintenance dose" of AHCC is appropriate. This is also where honesty is most important.
There is no published clinical protocol defining a maintenance dose of AHCC after HPV clearance. The commonly cited ranges — typically 500 to 1,000 mg per day — come from general AHCC immune support usage patterns and from integrative clinical practice, not from HPV-specific research. The only HPV-related trial studied 3 grams per day as the active dose. A reduced post-clearance dose has not been tested in a published HPV trial.
Some integrative practitioners do recommend a reduced dose during a transition period after clearance — for example, stepping down over one to two months before stopping entirely. This is a reasonable clinical approach, and it is not unsafe based on AHCC's established general safety profile developed over decades of use. But it should be clearly understood as clinical practice judgment, not evidence-based protocol.
If choosing to reduce rather than stop immediately, that is a defensible individual decision. It is not, however, a defined post-clearance protocol — and it should be made in consultation with a healthcare provider rather than based on general supplement guidance.
Who Might Benefit From Continuing Longer
While there is no universal recommendation to continue AHCC after HPV clearance, certain situations make a continued, time-limited period of use worth discussing with a provider.
-
High-risk strain with extended infection history. Individuals who cleared HPV 16 or HPV 18 after a prolonged infection — particularly those who had associated cellular changes — may benefit from a longer monitoring period and potentially from continued immune support during that window.
-
Multiple concurrent HPV strains. When the immune system was managing more than one HPV strain simultaneously before clearance, some practitioners consider a continued support period appropriate.
-
Unresolved immune suppressors. If the factors that may have contributed to a slow or difficult clearance — smoking, documented vitamin D deficiency, chronic high-stress — have not yet been fully addressed, continuing AHCC while actively working on those factors is a reasonable discussion to have with a provider.
-
Significant anxiety about re-infection. For some people, the psychological reassurance of continued supplementation during the first several months after clearance is a valid personal consideration. Anxiety itself can suppress immune function, and a decision that reduces that anxiety may have indirect benefit.
These are individual considerations, not clinical recommendations. Each person's situation is different, and a healthcare provider familiar with the full clinical history is the appropriate person to guide this decision.
Lifestyle After Clearance — What the Evidence Supports
The lifestyle factors that supported HPV clearance do not become irrelevant after a negative test result. Sustained immune function depends on sustained inputs — this is one of the most evidence-supported post-clearance principles, even if it is not HPV-specific.
-
Smoking cessation remains the highest-impact single change for cervical immune surveillance. Smoking impairs local immune responses in cervical tissue and is associated with persistent HPV infection. Stopping remains important after clearance.
-
Vitamin D optimization continues to matter. Adequate vitamin D levels support multiple arms of immune function. The NIH Office of Dietary Supplements notes that vitamin D plays a recognized role in immune regulation — maintaining adequate levels, particularly during winter months, is a reasonable ongoing priority.
-
Sleep quality and duration. Seven to nine hours of consistent sleep supports natural killer cell activity and broader immune maintenance. The immune benefit of adequate sleep does not stop at a negative test result.
-
Stress management. Cortisol-mediated immune suppression is a real and ongoing factor. Chronic high stress remains relevant to immune function after clearance, not only during active infection.
-
Nutritional support. Adequate folate, zinc, and vitamin C intake supports ongoing immune maintenance. These are not supplements to stop at clearance — they are part of sustained immune health.
For a detailed review of the lifestyle strategies that support HPV clearance and immune maintenance, the article on how to clear HPV naturally covers each of these factors in depth.

Lifestyle factors that supported HPV clearance continue to matter for immune maintenance after testing negative.
Continued Monitoring — What to Do Next
A negative HPV test result does not end the need for ongoing monitoring. This is one of the most important practical points for anyone who has recently cleared HPV.
Standard guidance from the WHO on HPV and cervical cancer emphasizes continued screening as a core component of cervical cancer prevention — a single negative result does not remove someone from the monitoring pathway.
Practical steps for post-clearance monitoring:
- Continue the screening schedule recommended by your healthcare provider. Do not self-discharge from monitoring based on a single negative result.
- Most providers recommend at least one confirmatory negative test before reducing monitoring frequency. The timing of that confirmatory test — typically 12 months after the initial negative — should be set by your provider based on your individual history.
- If you had CIN (cervical intraepithelial neoplasia or precancerous changes) alongside your HPV diagnosis, your provider may recommend more frequent follow-up regardless of current HPV status. Cellular changes have their own monitoring requirements independent of HPV detection.
- If you are uncertain what your next step should be — particularly regarding the interpretation of results — the article on HPV positive but normal Pap results explains how HPV status and cytology results interact, which is relevant context for understanding your monitoring pathway.
Monitoring is not a sign that something is wrong. It is the appropriate clinical response to having had HPV — and it continues to be appropriate after clearance.
Frequently Asked Questions
How do I know if my HPV is truly cleared?
HPV clearance is defined by a negative result on a standard HPV test, which detects active viral DNA in the sample. A single negative test is meaningful, but most providers recommend a confirmatory negative test — typically at the next scheduled screening interval — before considering the infection fully resolved. There is no test currently available that confirms the complete absence of latent HPV DNA in all cells. Clinical clearance, as measured by standard testing, is the accepted standard used in both clinical practice and research.
Should I retest after stopping AHCC?
Yes. Continuing your scheduled HPV screening after stopping AHCC is recommended regardless of how confident you feel about your clearance. A follow-up test at the interval your provider recommends — usually 12 months after a confirmed negative — provides the confirmatory data that supports reducing monitoring frequency. Stopping AHCC does not change the monitoring schedule; these are independent decisions.
Can I get HPV again after clearing it?
Yes. Prior clearance of one HPV infection does not provide immunity against future HPV exposure. Re-infection with the same strain or a different strain is possible through sexual contact. Consistent condom use reduces transmission risk but does not eliminate it. This is one reason why continued screening matters after clearance — not to create alarm, but to catch any new infection early, when it is most manageable.
Is a lower dose of AHCC enough for maintenance?
There is no published evidence defining what dose of AHCC, if any, is appropriate for maintenance after HPV clearance. The only HPV-specific clinical trial used 3 grams per day as the active dose. Lower doses used for general immune support are based on broader AHCC usage patterns, not HPV-specific research. If you are considering a reduced dose rather than stopping entirely, discuss that approach with your healthcare provider rather than selecting a dose based on general supplement guidance.
How long should I wait before stopping AHCC after a negative test?
There is no published protocol that defines this. Some integrative practitioners suggest continuing for one to two additional months after a confirmed negative result before stopping — allowing a transition period rather than an abrupt discontinuation. Others recommend stopping after confirmed clearance and relying on lifestyle factors and monitoring going forward. Both approaches are outside the published evidence base for HPV specifically. The decision should be made with your healthcare provider based on your individual history, the strain involved, and your current immune status.
Conclusion
Clearing HPV is a meaningful clinical outcome, and the question of whether to keep taking AHCC after clearing HPV is one that deserves a careful, honest answer rather than a reflexive one. The available evidence is reassuring — the Smith et al. trial found that clearance was sustained after AHCC was stopped — but it does not define a post-clearance protocol, and it does not address every individual situation.
Practical next steps:
- Confirm clearance with a follow-up test. Schedule the repeat HPV test your provider recommends — typically at 12 months — to establish a confirmed negative result before reducing monitoring frequency.
- Discuss the AHCC decision with your provider. Whether to stop, step down, or continue for a defined additional period depends on your strain history, immune status, and any ongoing risk factors. This is an individual decision, not a universal one.
- Maintain the lifestyle factors that supported clearance. Sleep, nutrition, stress management, and smoking cessation remain relevant to immune maintenance after clearance — these are the most evidence-supported post-clearance actions available.
- Stay on your monitoring schedule. Do not self-discharge from HPV screening based on a single negative result. Continued monitoring is the appropriate clinical response to having had HPV.
- Address any remaining immune suppressors. If smoking, chronic stress, or documented nutritional deficiencies contributed to your infection history, resolving those factors is the highest-value action available after clearance.
Related Reading

- Does AHCC really help clear HPV? A review of the research
- How long does AHCC take to clear HPV?
- Can HPV come back after clearance? What science really says
- AHCC for general longevity: immune resilience beyond HPV
References
- Smith JA et al. AHCC supplementation to support immune function to clear persistent HPV infections. Available at: PubMed — National Library of Medicine
- Centers for Disease Control and Prevention. HPV fact sheet. Available at: https://www.cdc.gov/hpv
- World Health Organization. Human papillomavirus (HPV) and cervical cancer. Available at: https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer
- National Institutes of Health — Office of Dietary Supplements. Vitamin D and immune function. Available at: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health







