


Nearly 80 million Americans are currently infected with HPV, according to the CDC — and for those in their reproductive years, a new diagnosis often triggers an immediate and understandable fear: will this affect my ability to have children? The honest answer is that, for most people, HPV does not directly prevent pregnancy or cause infertility. But the research does reveal specific, context-dependent concerns worth understanding clearly — without exaggeration and without dismissal.
Key Takeaways
- For most people, an HPV diagnosis does not significantly alter their fertility outlook or require delaying conception.
- The associations between HPV and female fertility outcomes — including implantation and miscarriage — are real but preliminary, observational, and do not establish causation.
- The most consistent fertility-related finding in the research involves HPV in semen and its association with reduced sperm motility and increased DNA fragmentation in male partners.
- Cervical treatments for HPV-related dysplasia (LEEP, cone biopsy) carry a small, established risk of preterm birth — the most clinically grounded fertility-adjacent concern linked to HPV.
- Supporting immune clearance of HPV before trying to conceive removes the variable entirely and is a reasonable, proactive step.
In This Article
The Short Answer
HPV does not directly cause infertility in the vast majority of people. For most individuals and couples trying to conceive, an HPV diagnosis alone is not a medical reason to delay pregnancy or to assume that fertility has been compromised.
The virus itself does not damage the ovaries, block the fallopian tubes, or disrupt ovulation. It does not prevent sperm from reaching an egg under normal circumstances. What the research does show is a set of more specific, context-dependent associations — in sperm quality, in implantation biology, in the outcomes of certain cervical procedures, and in assisted reproduction — that are worth knowing about. Understanding those nuances allows for informed conversations with healthcare providers rather than decisions driven by anxiety.
The sections below address each area honestly, including where the science is strong, where it is preliminary, and where it remains genuinely uncertain.
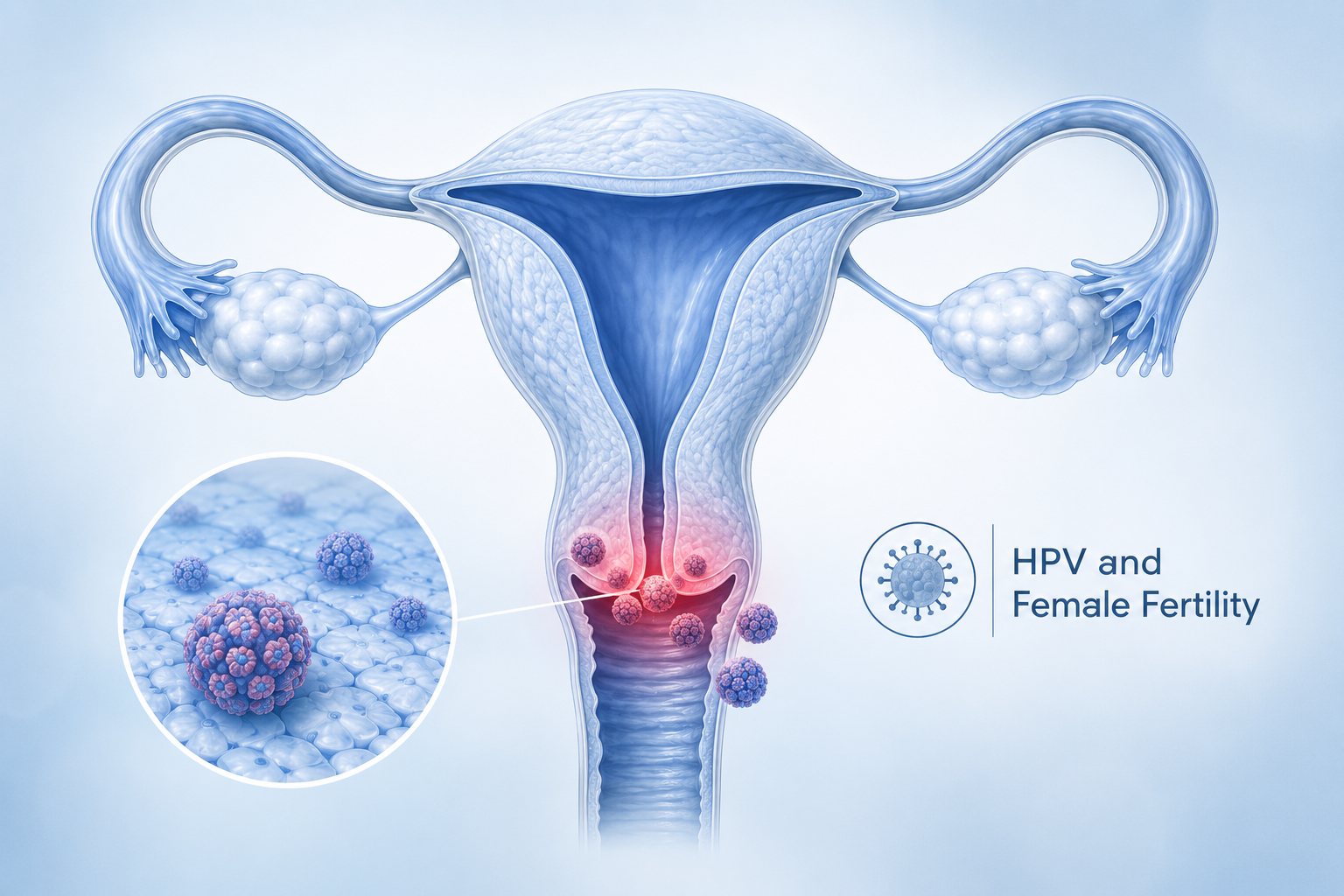
HPV and Female Fertility
The research on whether HPV can affect fertility in women is limited, largely observational, and — in several areas — inconsistent across studies. Three areas have received the most attention.
Implantation
Some laboratory and clinical studies suggest that HPV may interfere with trophoblastic cell function — the cells responsible for embedding an embryo into the uterine lining. A proposed mechanism involves HPV proteins interacting with endometrial receptors in ways that may impair implantation. However, these findings come from small studies with significant methodological limitations. The mechanism has not been established in large clinical populations, and the findings are inconsistent across studies. This remains an area of active investigation, not an established clinical concern.
Miscarriage
Several observational studies have found higher rates of early pregnancy loss in women with HPV infection, particularly with high-risk strains. A 2015 review by Pereira et al. examined the relationship between HPV, infertility, and assisted reproductive technology outcomes and noted these associations. It is important to be precise here: an association between HPV and miscarriage has been observed in some studies. That association does not establish that HPV causes miscarriage. Miscarriage is common — affecting roughly 10–20% of known pregnancies — and has many contributing factors. HPV may be one variable among many, but it has not been identified as a primary driver.
What this means practically
If you have HPV and are trying to conceive, the current evidence does not support the conclusion that your HPV status will prevent pregnancy or significantly increase your miscarriage risk. Discuss your full reproductive history with your OB/GYN or a reproductive specialist, who can assess your individual situation with appropriate clinical context.
How Cervical Treatments Affect Fertility
This is the most clinically established fertility concern associated with HPV — and it is important to note that it arises not from HPV itself, but from the procedures used to treat HPV-related cervical changes.
When high-risk HPV strains cause cervical intraepithelial neoplasia (CIN), treatment often involves removing the affected tissue. The two most common procedures are LEEP (loop electrosurgical excision procedure) and cone biopsy (conization). Both procedures are effective at removing precancerous cells, but they reduce the length of the cervix. A shorter cervix can slightly increase the risk of cervical incompetence and preterm birth in subsequent pregnancies.
What the evidence shows:
- The increased risk of preterm birth following LEEP or cone biopsy is real but small, and it depends significantly on how much tissue is removed.
- Most women who have undergone cervical treatment conceive without difficulty and deliver at term.
- The risk is higher with repeat procedures or when large amounts of tissue are removed.
- Women who have had cervical treatment and are planning a pregnancy should inform their OB/GYN so that cervical length can be monitored during pregnancy.
This is a reason to treat cervical dysplasia conservatively where clinically appropriate — not a reason to avoid treatment. Untreated high-grade dysplasia carries its own serious risks, including progression to cervical cancer. For more on how HPV-related cell changes can progress, see this detailed explanation of how HPV causes cancer.
The key action is communication: if you have had LEEP or cone biopsy, your prenatal care team needs to know.
HPV During Pregnancy
HPV is common among pregnant women, and in the majority of cases it does not harm the pregnancy or the developing baby. The immune changes that occur naturally during pregnancy — which temporarily suppress certain immune responses to protect the fetus — can sometimes allow HPV to become more active or for genital warts to grow more rapidly due to hormonal shifts. Treatment options for genital warts during pregnancy are more limited than outside of pregnancy, so early management before conception is preferable.
Vertical transmission
Transmission of HPV from mother to newborn during delivery can occur, though it is uncommon. The most established consequence of vertical transmission is recurrent respiratory papillomatosis (RRP) — a condition in which HPV-related warts develop in the throat and airways of infants or young children. RRP is rare, and most babies born to mothers with HPV do not develop it. Cesarean delivery is not routinely recommended as a preventive measure for HPV alone.
Practical guidance
Informing your obstetric provider of your HPV status is the appropriate course of action. Regular prenatal care, continued HPV monitoring, and open communication with your provider will allow for individualized management. HPV status alone is not a reason to alter delivery planning without specific clinical indication.
HPV and Male Fertility
When asking whether HPV can affect fertility, the male side of the equation has received growing research attention — and this is where the evidence is most consistent.
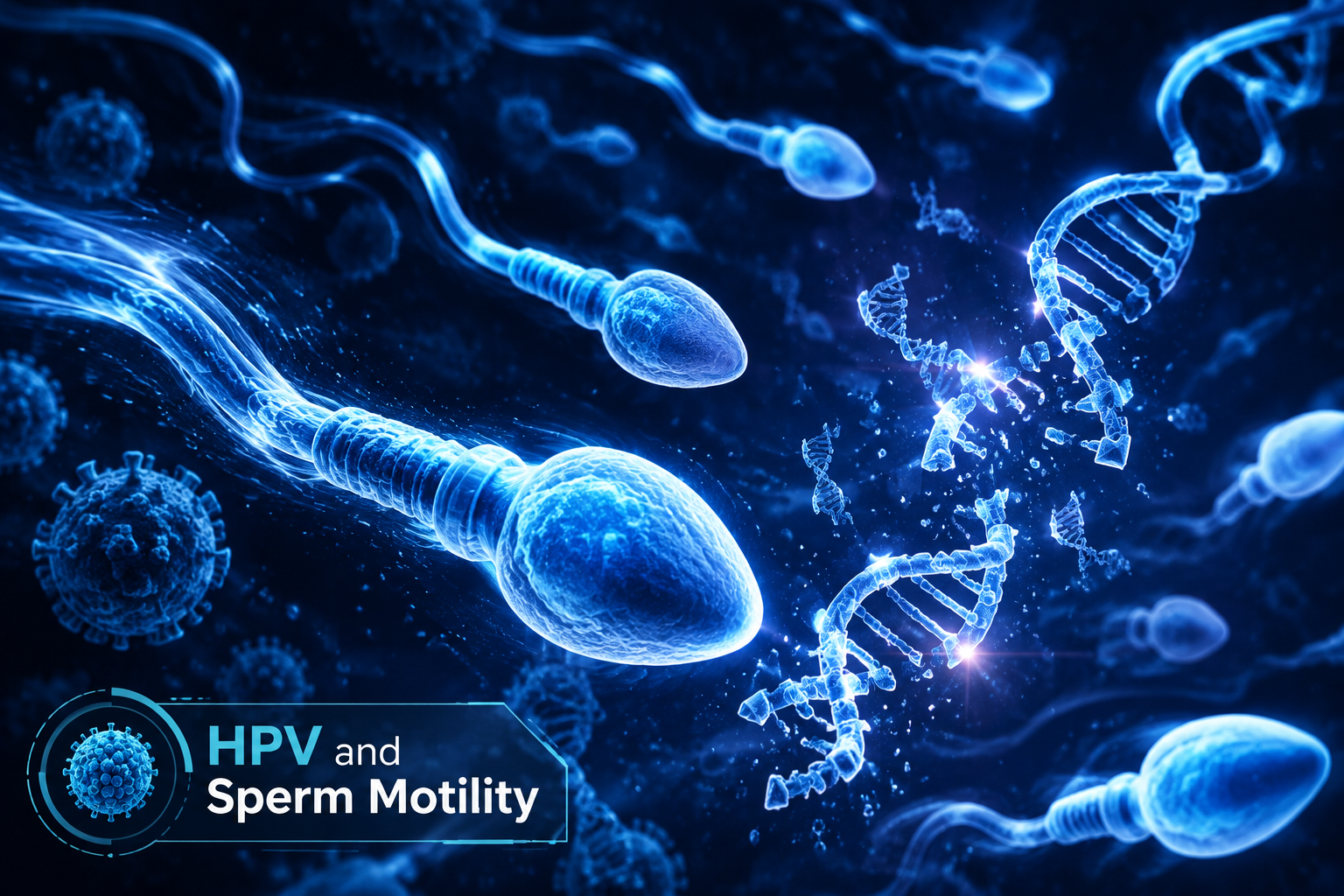
Multiple studies have found associations between HPV detected in semen and measurable changes in sperm parameters. A comprehensive 2024 review by Chenafi-Adham et al. examined the impact of HPV on both male and female fertility and identified the following associations in men:
- Reduced sperm motility — the most consistently reported finding across studies
- Increased sperm DNA fragmentation — HPV has been detected on sperm cells, particularly at the equatorial segment, where it may interfere with the sperm's ability to penetrate and fertilize an egg
- Reduced sperm count and viability in some, though not all, studies
- Anti-sperm antibody production — a proposed immune-mediated mechanism
The biological mechanism under investigation involves HPV binding directly to sperm cells. When HPV attaches to the equatorial segment of the sperm head, it may impair the cell's motility and its ability to complete fertilization. This is an area of active research, and not all studies agree on the magnitude of the effect.
What is clear is that HPV in men is not a benign bystander in reproductive health. Men are often unaware they carry HPV because there is no approved HPV test for men and symptoms are frequently absent. For a full overview of how HPV presents and behaves in men, see HPV in men: no symptoms, no test, still at risk.
If a couple is experiencing unexplained fertility challenges and the male partner has not been evaluated for HPV, this is worth raising with a reproductive specialist.
HPV and IVF Outcomes
For couples undergoing in vitro fertilization (IVF) or other forms of assisted reproductive technology (ART), some studies suggest that HPV infection in either partner may reduce success rates. The proposed pathways include effects on sperm quality, embryo development, and endometrial implantation — each of which has been discussed in the sections above.
The evidence in this area is preliminary. Study populations are small, methodologies vary, and many confounding factors — including age, sperm quality, uterine factors, and the specific HPV strain involved — make it difficult to isolate HPV's contribution. The Pereira et al. review noted that HPV-positive sperm may be associated with lower fertilization rates in IVF cycles, though this finding has not been consistently replicated.
If you or your partner have HPV and are planning IVF, the appropriate step is to disclose HPV status to your reproductive endocrinologist. They can factor this into protocol planning and monitoring. This article does not provide IVF clinical guidance — that conversation belongs with a qualified reproductive specialist who knows your full medical history.
What You Can Do
An HPV diagnosis while trying to conceive does not require panic or inaction. The steps below are practical, evidence-informed, and applicable to most people in this situation.

| Action | Who It Applies To | Why It Matters |
|---|---|---|
| Continue regular HPV monitoring (Pap/HPV co-testing) | Everyone with HPV | Catches dysplasia early before treatment is needed |
| Inform your fertility specialist of HPV status | Anyone undergoing IVF or ART | Enables informed protocol decisions |
| Inform your OB/GYN of prior cervical treatment | Anyone who has had LEEP or cone biopsy | Allows cervical length monitoring during pregnancy |
| Support immune clearance through lifestyle | Everyone | A cleared infection removes the variable entirely |
| Do not delay conception for HPV alone | Most people without active dysplasia | HPV alone rarely requires a fertility delay |
| Ask male partner about HPV evaluation | Couples with unexplained fertility challenges | HPV in semen may affect sperm parameters |
For those wondering why HPV sometimes persists despite efforts to clear it, understanding the immune factors involved is genuinely useful. The article on why HPV does not clear in some people covers the biological and lifestyle reasons in detail.
For a broader overview of natural strategies that support the immune system's ability to suppress HPV, the guide on how to clear HPV naturally is a practical starting point.
Supporting HPV Clearance Before Trying to Conceive
Clearing HPV before trying to conceive removes the variable entirely. The immune system is the primary mechanism by which the body suppresses and eventually clears HPV — and there are well-established lifestyle factors that support that process.

Foundational immune support steps:
- Smoking cessation — smoking is one of the most consistently identified factors associated with HPV persistence and cervical dysplasia progression
- Vitamin D optimization — vitamin D plays a documented role in immune regulation, and deficiency is common; a blood test can identify whether supplementation is appropriate
- Sleep quality — chronic sleep deprivation measurably impairs immune surveillance
- Stress reduction — chronic psychological stress suppresses the immune responses most relevant to viral clearance
AHCC and HPV clearance
Among supplements studied for HPV support, AHCC (Active Hexose Correlated Compound) is the only one with a published, placebo-controlled human clinical trial specifically targeting HPV clearance. The research was conducted by Dr. Judith Smith at the University of Texas Health Science Center at Houston, using a protocol of 3 grams per day taken on an empty stomach for a minimum of six months. The findings are promising and preliminary — this is not an established cure, and results vary between individuals.
For a detailed review of the clinical evidence behind AHCC and HPV, see does AHCC really help clear HPV. For protocol specifics, the article on what dosage of AHCC to take for HPV covers the clinical study parameters in detail.
NovaHerbs AHCC provides 700 mg per capsule, manufactured in the USA in a GMP-certified facility. At the research-validated dose of 3 grams per day, this corresponds to approximately 4–5 capsules daily taken on an empty stomach. AHCC is relevant here solely as immune support for HPV clearance — there is no clinical evidence that it improves fertility or protects against miscarriage, and it should not be framed that way.
Frequently Asked Questions
Can I get pregnant if I have HPV?
Yes. HPV does not directly block conception. The virus does not damage the ovaries, fallopian tubes, or the uterus in ways that prevent pregnancy from occurring. The majority of people with HPV conceive without difficulty. The specific concerns discussed in this article — sperm quality, implantation associations, cervical treatment effects — are real but context-dependent and affect a minority of people. An HPV diagnosis alone is not a medical reason to delay trying to conceive.
Does HPV cause miscarriage?
HPV does not cause miscarriage as an established clinical fact. Some observational studies have found higher miscarriage rates among women with HPV, particularly high-risk strains, but these studies show association — not causation. Miscarriage is common and has many contributing factors. The current evidence is not strong enough to conclude that HPV is a meaningful driver of pregnancy loss for most people. Discuss your individual history and risk factors with your OB/GYN.
Can HPV affect my partner's sperm?
Several studies suggest it can. HPV detected in semen has been associated with reduced sperm motility, increased DNA fragmentation, and in some studies, lower sperm count. The most consistent finding across the research is reduced motility, potentially linked to HPV binding to the equatorial segment of sperm cells. This does not mean that a man with HPV cannot father a child — but it is a relevant variable for couples experiencing unexplained fertility challenges, and worth raising with a reproductive specialist.
Should I wait until HPV clears before trying to conceive?
For most people, no. HPV alone is not a standard medical reason to delay conception. The decision to wait should be based on your specific clinical situation — for example, if you have active high-grade cervical dysplasia that requires treatment, it is generally advisable to complete that treatment and allow healing before pregnancy. If you simply have a positive HPV test without dysplasia, delaying conception is not typically recommended. Discuss your individual situation with your healthcare provider.
Does HPV affect IVF success rates?
Some studies suggest HPV in either partner may reduce IVF success rates, potentially through effects on sperm quality, embryo development, and implantation. However, this evidence is preliminary, inconsistent across studies, and complicated by many confounding variables. If you are undergoing IVF and have HPV, disclose this to your reproductive endocrinologist so they can incorporate it into your care plan. Do not make decisions about IVF based on this article alone — that conversation requires a specialist with full knowledge of your reproductive history.
Conclusion
HPV and fertility is a topic where anxiety often outpaces the actual evidence. The core message of this article is worth restating clearly: for most people, HPV does not directly cause infertility, and an HPV diagnosis alone is not a reason to stop trying to conceive or to assume that pregnancy is out of reach.
The real concerns are more specific. Sperm quality in HPV-positive men is the most consistently documented fertility-adjacent finding in the research. Cervical treatment procedures carry a small, established risk of preterm birth. Associations with implantation and miscarriage exist in observational data but have not been proven causal. IVF outcomes may be modestly affected in some cases. Each of these concerns is manageable with the right clinical oversight.
Concrete next steps:
- Talk to your provider — inform your OB/GYN, fertility specialist, or reproductive endocrinologist of your HPV status and any prior cervical treatments. This is the single most important action.
- Continue HPV monitoring — regular Pap and HPV co-testing allows early detection of any cervical changes before they require intervention.
- Address modifiable immune factors — quit smoking if applicable, optimize vitamin D levels, prioritize sleep, and reduce chronic stress. These steps support HPV clearance and overall reproductive health.
- Consider immune support — if you are not yet trying to conceive and want to support HPV clearance first, review the clinical evidence for AHCC and discuss supplementation with your provider.
- Do not delay unnecessarily — if your HPV status is uncomplicated (positive test, no dysplasia), work with your provider to confirm that conception can proceed on your intended timeline.
Related Reading
- For men navigating an HPV diagnosis with no symptoms and no available test, HPV in men: what you need to know covers the full picture.
- If HPV has persisted despite time and lifestyle changes, why HPV does not clear in some people explains the biological and behavioral factors involved.
- For a thorough review of the clinical research behind AHCC as an immune support tool for HPV, does AHCC really help clear HPV is the definitive starting point.
- To understand the full spectrum of natural strategies that support the immune system's ability to suppress HPV, how to clear HPV naturally offers a practical, evidence-referenced overview.
References
- Chenafi-Adham S, et al. Impact of HPV on Male and Female Fertility. Pathogens. 2024;13(12):1076. PMC11728800. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11728800/
- Pereira N, et al. Human Papillomavirus Infection, Infertility, and Assisted Reproductive Outcomes. Journal of Pathogens. 2015. PMC4644557. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4644557/
- Centers for Disease Control and Prevention. HPV Fact Sheet. https://www.cdc.gov/hpv
- National Institutes of Health Office of Dietary Supplements. Vitamin D: Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- PubMed — AHCC clinical research index. https://pubmed.ncbi.nlm.nih.gov/
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Consult your healthcare provider before beginning any new supplement regimen.
By Dr. Zafer Atli | Integrative Medicine & Women's Health
